
10.5: Lower Gastrointestinal Tract
- Page ID
- 30687

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Figure \(\PageIndex{1}\) shows some of the cells of what has been called “the last human organ to be discovered.” This “organ” weighs about 200 grams (0.44 lb.) and consists of a hundred trillion cells, yet scientists are only now beginning to learn everything it does and how it varies among individuals. What is it? It’s the mass of bacteria that live in our lower gastrointestinal tract.
Organs of the Lower Gastrointestinal Tract
Most of the bacteria that normally live in the lower gastrointestinal (GI) tract live in the large intestine. They have important and mutually beneficial relationships with the human organism. We provide them with a great place to live, and they provide us with many benefits, some of which you can read about below. Besides the large intestine and its complement of helpful bacteria, the lower GI tract also includes the small intestine. The latter is arguably the most important organ of the digestive system. It is where most chemical digestion and virtually all absorption of nutrients take place.
Small Intestine
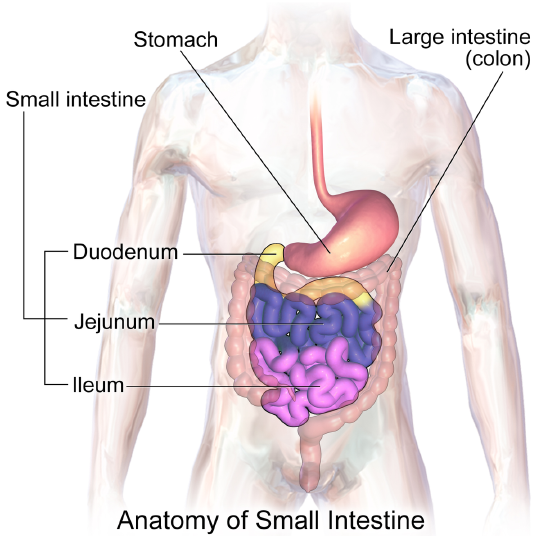
The small intestine (also called the small bowel or gut) is the part of the GI tract between the stomach and large intestine. Its average length in adults is 4.6 m (15 ft) in females and 6.9 m (22 ft 8 in.) in males. It is approximately 2.5 to 3.0 cm (1.0 to 1.2 in.) in diameter (it is called “small” because it is much smaller in diameter than the large intestine). The internal surface area of the small intestine totals an average of about 30 m2 (323 ft2). Structurally and functionally, the small intestine can be divided into three parts, called the duodenum, jejunum, and ileum, as shown in Figure \(\PageIndex{2}\) and described below.
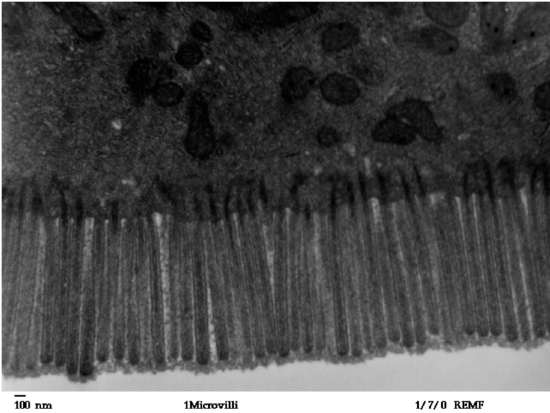
The mucosa lining the small intestine is very wrinkled and covered with finger-like projections called villi. In fact, each square inch of mucosa contains around 20,000 villi. The individual cells on the surface of the villi also have many finger-like projections, the microvilli shown in Figure \(\PageIndex{3}\). There are thought to be well over 100 billion microvilli per square inch of intestinal mucosa! All of these wrinkles, villi, and microvilli greatly increase the surface area for chyme to come into contact with digestive enzymes, which coat the microvilli, as well as forming a tremendous surface area for the absorption of nutrients. Inside each of the villi is a network of tiny blood and lymph vessels that receive the absorbed nutrients and carry them away in the blood or lymph circulation. The wrinkles and projections in the intestinal mucosa also slow down the passage of chyme so there is more time for digestion and absorption to take place.
Duodenum
The duodenum is the first part of the small intestine, directly connected to the stomach. It is also the shortest part of the small intestine, averaging only about 25 cm (10 in.) in length in adults. Its main function is chemical digestion, and it is where most of the chemical digestion in the entire GI tract takes place.
.jpg?revision=1&size=bestfit&width=520&height=283)
The duodenum receives partially digested, semi-liquid chyme from the stomach. It receives digestive enzymes and alkaline bicarbonate from the pancreas through the pancreatic duct, and it receives bile from the liver via the gallbladder through the common bile duct (Figure \(\PageIndex{4}\)). In addition, the lining of the duodenum secretes digestive enzymes and contains glands — called Brunner’s glands — that secrete mucus and bicarbonate. The bicarbonate from the pancreas and Brunner’s glands as well as bile from the liver neutralize the highly acidic chyme after it enters the duodenum from the stomach. This is necessary because the digestive enzymes in the duodenum require a nearly neutral environment in order to work. The three major classes of compounds that undergo chemical digestion in the duodenum are carbohydrates, proteins, and lipids.
Digestion of Carbohydrates in the Duodenum
Complex carbohydrates such as starches are broken down by the digestive enzyme amylase from the pancreas to short-chain molecules consisting of just a few saccharides (that is, simple sugars). Disaccharides, including sucrose and lactose, are broken down into simple sugars by duodenal enzymes: sucrase breaks down sucrose, and lactase (if present) breaks down lactose. Some carbohydrates are not digested in the duodenum and ultimately pass undigested to the large intestine, where they may be digested by intestinal bacteria.
Digestion of Proteins in the Duodenum
In the duodenum, the pancreatic enzymes trypsin and chymotrypsin cleave proteins into peptides. Then, these smaller molecules are broken down into amino acids. Their digestion is catalyzed by pancreatic enzymes called peptidases.
Digestion of Lipids in the Duodenum
Pancreatic lipase breaks down triglycerides into fatty acids and glycerol. Lipase works with the help of bile secreted by the liver and stored in the gall bladder. Bile salts attach to triglycerides to help them emulsify or form smaller particles (called micelles) that can disperse through the watery contents of the duodenum. This increases the access to the molecules by pancreatic lipase.
Jejunum
The jejunum is the middle part of the small intestine, connecting the duodenum and the ileum. The jejunum is about 2.5 m (8.2 ft) long. Its main function is the absorption of the products of digestion, including sugars, amino acids, and fatty acids. Absorption occurs by simple diffusion (water and fatty acids), facilitated diffusion (the simple sugar fructose), or active transport (amino acids, small peptides, water-soluble vitamins, and most glucose). All nutrients are absorbed into the blood except for fatty acids and fat-soluble vitamins, which are absorbed into the lymph. Although most nutrients are absorbed in the jejunum, there are a few exceptions:
- Iron is absorbed in the duodenum.
- Vitamin B12 and bile salts are absorbed in the ileum.
- Water and lipids are absorbed throughout the small intestine, including the duodenum and ileum in addition to the jejunum.
Ileum
The ileum is the third and final part of the small intestine, directly connected at its distal end to the large intestine. The ileum is about 3 m (9.8 ft) long. Some cells in the lining of the ileum secrete enzymes that catalyze the final stages of digestion of any undigested protein and carbohydrate molecules. However, the main function of the ileum is to absorb vitamin B12 and bile salts. It also absorbs any other remaining nutrients that were not absorbed in the jejunum. All substances in chyme that remain undigested or unabsorbed by the time they reach the distal end of the ileum pass into the large intestine.
Large Intestine
The large intestine, also called the large bowel, is the last organ of the GI tract. In adults, it averages about 1.5 m (5 ft) in length. It is shorter than the small intestine but at least twice as wide, averaging about 6.5 cm (2.5 in.) in diameter. Water is absorbed from the chyme as it passes through the large intestine, turning the chyme into solid feces. Feces is stored in the large intestine until it leaves the body during defecation.
Parts of the Large Intestine
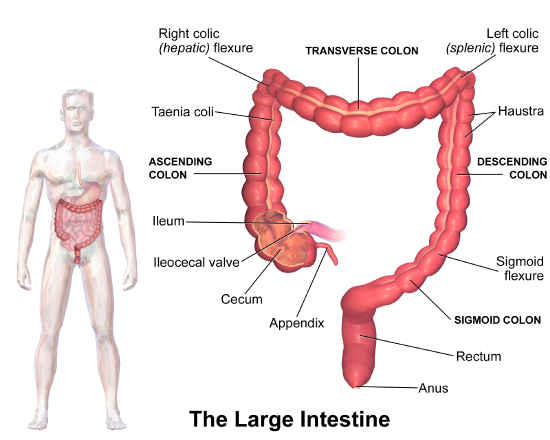
Like the small intestine, the large intestine can be divided into several parts, as shown in Figure \(\PageIndex{5}\). The large intestine begins at the end of the small intestine, where a valve separates the small and large intestines and regulates the movement of chyme into the large intestine. The first part of the large intestine, where chyme enters from the small intestine, is called the cecum. From the cecum, the large intestine continues upward as the ascending colon, travels across the upper abdomen as the transverse colon, and then continues downward as the descending colon. It then becomes a V-shaped region called the sigmoid colon, which is attached to the rectum. The rectum stores feces until elimination occurs. It transitions to the final part of the large intestine, called the anus, which has an opening to the outside of the body for feces to pass through.
A projection from the cecum of the colon is known as the appendix. The function of the appendix is uncertain, but it does not seem to be involved in digestion or absorption. It may play a role in immunity, and in the fetus, it seems to have an endocrine function, releasing hormones needed for homeostasis. Some biologists speculate that the appendix may also store a sample of the colon’s normal bacteria. If so, it may be able to repopulate the colon with the bacteria if illness or antibiotic medications deplete these microorganisms. Appendicitis, or infection and inflammation of the appendix, is a fairly common medical problem, typically resolved by surgical removal of the appendix (appendectomy). People who have had their appendix surgically removed do not seem to suffer any ill effects, so the organ is considered to be dispensable. As such, it is often referred to as a vestigial organ, which is a previously useful organ that has been retained over evolutionary time as part of the anatomy, even though it no longer has a function in the body.
Functions of the Large Intestine
The removal of water from chyme to form feces starts in the ascending colon and continues throughout much of the length of the organ. Salts such as sodium are also removed from food wastes in the large intestine before the wastes are eliminated from the body. This allows salts as well as water to be recycled in the body.
The large intestine is also the site where huge numbers of beneficial bacteria ferment many unabsorbed materials in food waste. The bacterial breakdown of undigested polysaccharides produces nitrogen, carbon dioxide, methane, and other gases that are responsible for intestinal gas, or flatulence. These bacteria are particularly prevalent in the descending colon. Some of the bacteria also produce vitamins that are absorbed from the colon. The vitamins include vitamins B1 (thiamine), B2 (riboflavin), B7 (biotin), B12, and K. Another role of bacteria in the colon is immune function. The bacteria may stimulate the immune system to produce antibodies that are effective against similar, but pathogenic, bacteria, thereby preventing infections. Still, other roles played by bacteria in the large intestine include breaking down toxins before they can poison the body, producing substances that help prevent colon cancer, and inhibiting the growth of harmful bacteria.
Colorectal cancer, or cancer of the colon or rectum, is the fourth most common cancer in the United States. It is also the second most common cause of cancer deaths in this country. Widespread screening of patients for signs of colorectal cancer has significantly lowered the death rate in recent years. Because early-stage colorectal cancer is usually asymptomatic, routine screening is important for identifying cancer early when chances of a cure are still high.
Screening for colorectal cancer has also become easier and less invasive in recent years. One way to test for colorectal cancer is to examine a sample of stool and look for occult (hidden from the unaided eye) blood in the stool. This test is based on the assumption that blood vessels in cancer are fragile and may be easily damaged by the passage of feces through the colon or rectum. The damaged vessels may bleed into the feces but rarely bleed enough for blood to be visible in the stool. Stool for the occult blood test can be collected by the patient at home with a test kit provided by a doctor. If occult blood is detected in the stool, a different type of follow-up test is generally needed to determine whether cancer is the cause of the bleeding.
A similarly simple and noninvasive but more definitive test for colorectal cancer looks for DNA from cancer cells in the stool. Again, the patient can collect the stool sample at home using a simple test kit and mail the specimen to a lab, which does the analysis. If the test comes back positive, then a direct visual examination of the colon and rectum by colonoscopy is required.
Colonoscopy is the gold standard for the diagnosis of colorectal cancer. Using a tiny camera at the end of a long tube inserted up into the colon, a doctor can directly visualize the lining of the large intestine and spot any suspicious areas that may be cancerous. While a colonoscopy is invasive and requires the patient to prepare for the test for a couple of days by changing his or her diet and drinking special fluids, it reveals more than just cancer. A colonoscopy also reveals any growths called polyps in the colon. Colon polyps are not cancer but often develop into cancerous lesions, so if they are found during a colonoscopy, a surgical instrument inserted with the scope is usually used to remove them. Therefore, a colonoscopy can not only detect cancer in its early stages, but it can even help prevent cancer by enabling the removal of potentially pre-cancerous polyps.
A test similar to colonoscopy may be done in some patients. Called a flexible sigmoidoscopy, it allows a doctor to use a small camera to inspect the rectum and lower third of the colon, where the majority of cases of colorectal cancer occur. However, the rest of the colon cannot be examined with a sigmoidoscopy. Another alternative to a full-blown colonoscopy is a virtual colonoscopy, in which a CT scan of the rectum and colon is used to make detailed cross-sectional images of the organs. The images can then be studied by a specialist to detect cancers or polyps. For both of these colonoscopy alternatives, a follow-up colonoscopy is required if polyps or potentially cancerous lesions are detected.
Unless you have a family history of colorectal cancer or certain other risk factors, you probably do not need to start routine screening for the disease until middle age. Your doctor can tell you the most appropriate starting age for your particular case, given your risk factors and current cancer guidelines. You may be able to be screened with one of the less invasive methods rather than colonoscopy until you are somewhat older. Again, check with your doctor for specific recommendations. All of the testing methods have pros and cons that should be taken into consideration by a given patient and medical provider.
Review
- Which organs are included in the lower GI tract?
- Name the parts of the small intestine.
- How is the mucosa of the small intestine specialized for digestion and absorption?
- What digestive substances are secreted into the duodenum, and what compounds in food do they help digest?
- What is the main function of the jejunum?
- What roles are played by the ileum?
- Name the parts of the large intestine.
- Identify the main functions of the large intestine.
- How do beneficial bacteria in the large intestine help the human organism?
- True or False. The first part of the large intestine is where most chemical digestion takes place.
- True or False. The small intestine is actually longer than the large intestine.
- When diarrhea occurs, feces leaves the body in a more liquid state than normal. What part of the digestive system do you think is involved in diarrhea? Explain your answer.
- Arrange the following parts of the lower GI tract in order of how food passes through them, from earliest to latest. Note that not all parts are listed.
cecum; duodenum; sigmoid colon; jejunum; rectum; ileum
- Which enzyme digests proteins?
A. trypsin
B. amylase
C. lipase
D. lactase
- What is intestinal gas, or flatulence, due to?
Explore More
Did you know you have about 100 million neurons in your intestines? In this fascinating TED talk, food scientist Heribert Watzke talks about the "hidden brain" in our gut and the surprising things it makes us feel.
Attributions
- Bacteroides biacutis by US government, Public Domain via Wikimedia Commons
- Small intestine anatomy by Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. CC BY 3.0 via Wikimedia Commons
- Human jejunum microvilli by Louisa Howard, Katherine Connollly, Public Domain via Wikimedia Commons
- biliary tract medium by www.6xc.com.au6XC, CC BY-NC-ND 4.0
- Large intestine by Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. CC BY 3.0 via Wikimedia Commons
- Text adapted from Human Biology by CK-12 licensed CC BY-NC 3.0