
22.8: Functions of the Female Reproductive System
- Page ID
- 17795

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)A mother-to-be waits patiently for her fetus to grow as her belly swells. Reproduction is all about making babies, and the female reproductive system is specialized for this purpose. Its functions include producing gametes called eggs, secreting sex hormones (such as estrogen), providing a site for fertilization, gestating a fetus if fertilization occurs, giving birth to a baby, and breastfeeding a baby after birth. The only thing missing is sperm.

Egg Production
At birth, ovaries contain all the eggs that will ever be produced, which may include a million or more eggs. The eggs don't start to mature, however, until a female enters puberty and attains sexual maturity. After that, one egg typically matures each month and is released from an ovary. This continues until menopause (cessation of monthly periods), typically by age 52. By then, viable eggs may be almost depleted, and hormone levels can no longer support the monthly cycle. During the reproductive years, which of the two ovaries releases an egg in a given month seems to be a matter of chance. Occasionally, both ovaries will release an egg at the same time. If both eggs are fertilized, the offspring are fraternal twins (dizygotic, or "two-zygote," twins), and they are no more alike genetically than non-twin siblings.
Oogenesis
The process of producing eggs in the ovaries of a fetus carrying XX chromosomes is called oogenesis. Eggs are haploid gametes, and their production occurs in several steps that involve different types of cells, as summarized in Figure \(\PageIndex{2}\). Oogenesis is completed long before birth. It occurs when diploid germ cells called oogonia (singular, oogonium) undergo mitosis. Each such cell division produces two diploid cells. One is called the primary oocyte, and the other is retained to help maintain a reserve of oogonia. The primary oocyte, in turn, starts to go through the first cell division of meiosis (meiosis I). However, it does not complete meiosis I until puberty.
.jpg?revision=1&size=bestfit&width=637&height=534)
Maturation of a Follicle
Beginning in puberty, about once a month, one of the follicles in an ovary undergoes maturation, and an egg is released. As the follicle matures, it goes through changes in the numbers and types of its cells. The primary oocyte within the follicle also resumes meiosis. It completes meiosis I, which began long before birth, to form a secondary oocyte and a smaller cell, called the first polar body. Both the secondary oocyte and the first polar body are haploid cells. The secondary oocyte has most of the cytoplasm from the primary oocyte and is much larger than the first polar body, which soon disintegrates and disappears. The secondary oocyte begins meiosis II, but only completes it if the egg is fertilized.
Release of an Egg
It typically takes 12 to 14 days for a follicle to mature in an ovary and for the secondary oocyte to form. Then, the follicle bursts open and the ovary ruptures, releasing the secondary oocyte from the ovary. This event is called ovulation. The now-empty follicle starts to change into a structure called a corpus luteum. The expelled secondary oocyte is usually swept into the nearby Fallopian tube by its waving, fingerlike fimbriae.
Uterine Changes
While the follicle matures in the ovary, the uterus also changes to prepare it for an embryo if fertilization occurs. For example, the endometrium gets thicker and becomes more vascular. Around ovulation, the cervix undergoes changes that help sperm reach the oocyte to fertilize it. The cervical canal widens, and the cervical mucus becomes thinner and more alkaline. These changes help promote the passage of sperm from the vagina into the uterus and make the environment more hospitable to sperm.
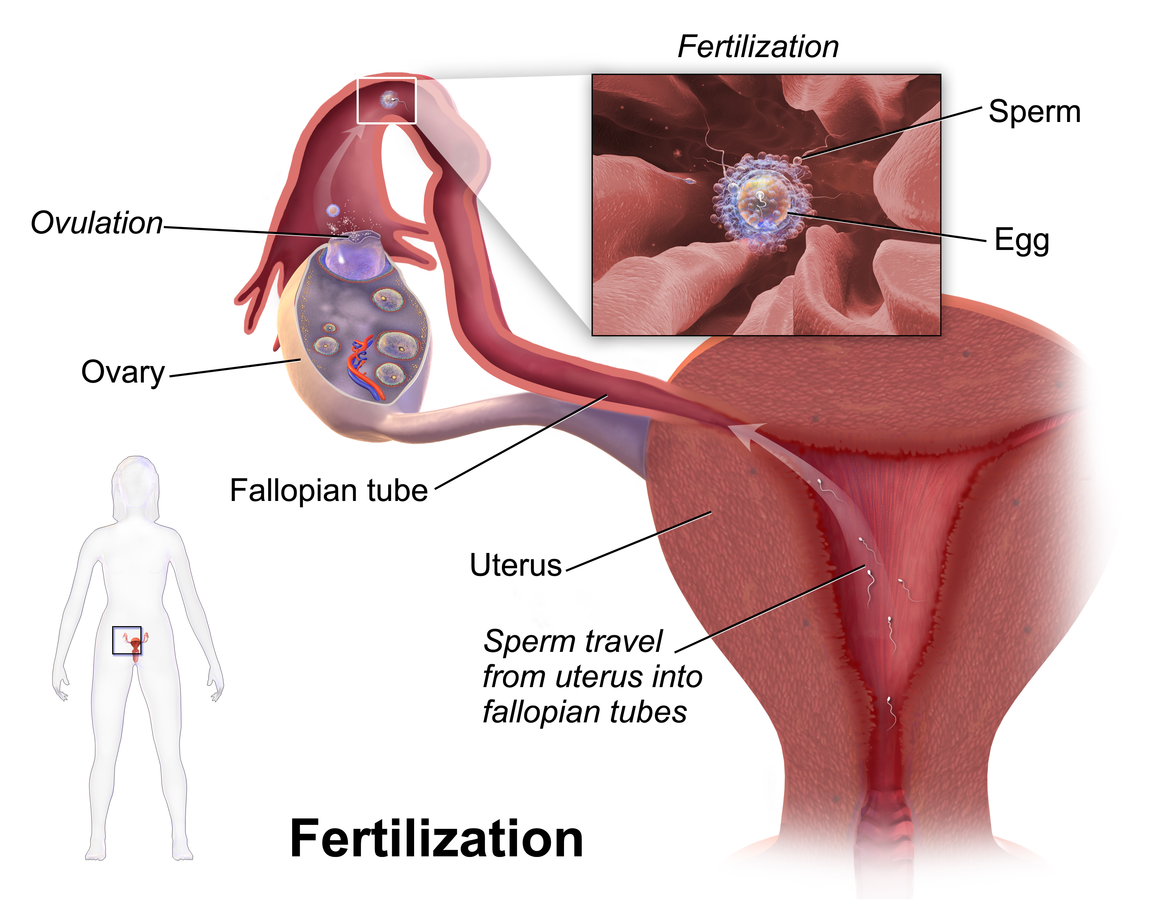
Fertilization — or Not
Fertilization of an egg by a sperm normally occurs in a Fallopian tube, most often in the part of the tube that passes above the ovary (Figure \(\PageIndex{3}\)). In order for fertilization to occur, sperm must “swim” from the vagina where they are deposited, through the cervical canal to the uterus and then through the body of the uterus to one of the Fallopian tubes. Once sperm enter a Fallopian tube, tubular fluids help carry them through the tube toward the secondary oocyte at the other end. The secondary oocyte also functions to promote fertilization. It releases molecules that guide the sperm and allow the surface of the egg to attach to the surface of the sperm. The egg can then absorb the sperm, allowing fertilization to occur.
If Fertilization Occurs
If the secondary oocyte is fertilized by a sperm as it passes through the Fallopian tube, the secondary oocyte quickly completes meiosis II, forming a diploid zygote and another polar body. (This second polar body, like the first, normally breaks down and disappears.) The zygote then continues the journey through the fallopian tube to the uterus, during which it undergoes several mitotic cell divisions. When it reaches the uterus, up to five days after fertilization, it consists of a ball of cells called a blastocyst. Within another day or two, the blastocyst implants itself in the endometrium lining the uterus, and gestation begins.
If Fertilization Does Not Occur
What happens if the secondary oocyte is not fertilized by a sperm as it passes through the Fallopian tube? It continues on its way to the uterus without ever completing meiosis II. It is likely to disintegrate within a few days while still in the Fallopian tube. Any remaining material will be shed from the woman’s body during the next menstrual period.
Pregnancy
Pregnancy is the carrying of one or more offspring from fertilization until birth. This is one of the major functions of the female reproductive system. It involves virtually every other body system, including the cardiovascular, urinary, and respiratory systems, to name just three. The maternal organism plays a critical role in the development of the offspring. They must provide all the nutrients and other substances needed for the normal growth and development of the offspring and remove the wastes excreted by the offspring. Most nutrients are needed in greater amounts by a pregnant individual to meet fetal needs, but some are especially important, including folic acid, calcium, iron, and omega-3 fatty acids. A healthy diet and prenatal vitamin supplements are recommended for the best pregnancy outcome. A pregnant person should also avoid ingesting substances (such as alcohol) that can damage the developing offspring, especially early in the pregnancy when all of the major organs and organ systems are forming.
When counted from the first day of the last menstrual period, the average duration of pregnancy is about 40 weeks (38 weeks when counted from the time of fertilization). However, a pregnancy that lasts between 37 and 42 weeks is still considered within the normal range. From the point of view of the maternal organism, the total duration of pregnancy is typically divided into three periods, called trimesters, each of which lasts about three months. This division of the total period of gestation is useful for summarizing the typical changes during pregnancy. From the point of view of the developing offspring, however, the major divisions are different. They are the embryonic and fetal stages. The offspring is called an embryo from the time it implants in the uterus through the first eight weeks of life. After that, it is called a fetus for the duration of the pregnancy.
First Trimester
The first trimester begins at the time of fertilization and lasts for the next 12 weeks. Even before a pregnant person knows they are pregnant, they may experience signs and symptoms of pregnancy. They may notice a missed menstrual period, and they may also experience a tender nipple area, increased appetite, and more frequent urination. Many individuals also experience nausea and vomiting in the first trimester. This is often called “morning sickness” because it commonly occurs in the morning but may occur at any time of day. Some lose weight during the first trimester because of morning sickness.
Second Trimester
The second trimester occurs during weeks 13 to 28 of pregnancy. A pregnant person may feel more energized during this trimester. If she experienced nausea and vomiting during the first trimester, these symptoms often subside during the second trimester. Weight gain starts occurring during this trimester, as well. By about week 20, the fetus is getting large enough that the mother can feel its movements. The photo on the left in Figure \(\PageIndex{4}\) shows a pregnant woman at week 26, toward the end of the second trimester. (For comparison, the same woman is shown on the right of Figure \(\PageIndex{4}\) at the end of the third trimester.)
Third Trimester
The third trimester occurs during weeks 29 through birth (at about 40 weeks). During this trimester, the uterus expands rapidly, making up a larger and larger portion of the woman's abdomen. Weight gain is also more rapid. During the third trimester, the movements of the fetus become stronger and more frequent, and they may become disruptive to the mother. As the fetus grows larger, its weight and the space it takes up may lead to symptoms in the mother such as back pain, swelling of the lower extremities, more frequent urination, varicose veins, and heartburn. By the end of the third trimester, the woman's abdomen often will transform in shape as it drops, due to the fetus turning to a downward position before birth so its head rests on the cervix. This relieves pressure on the upper abdomen, but reduces bladder capacity and increases pressure on the pelvic floor and rectum.

Childbirth
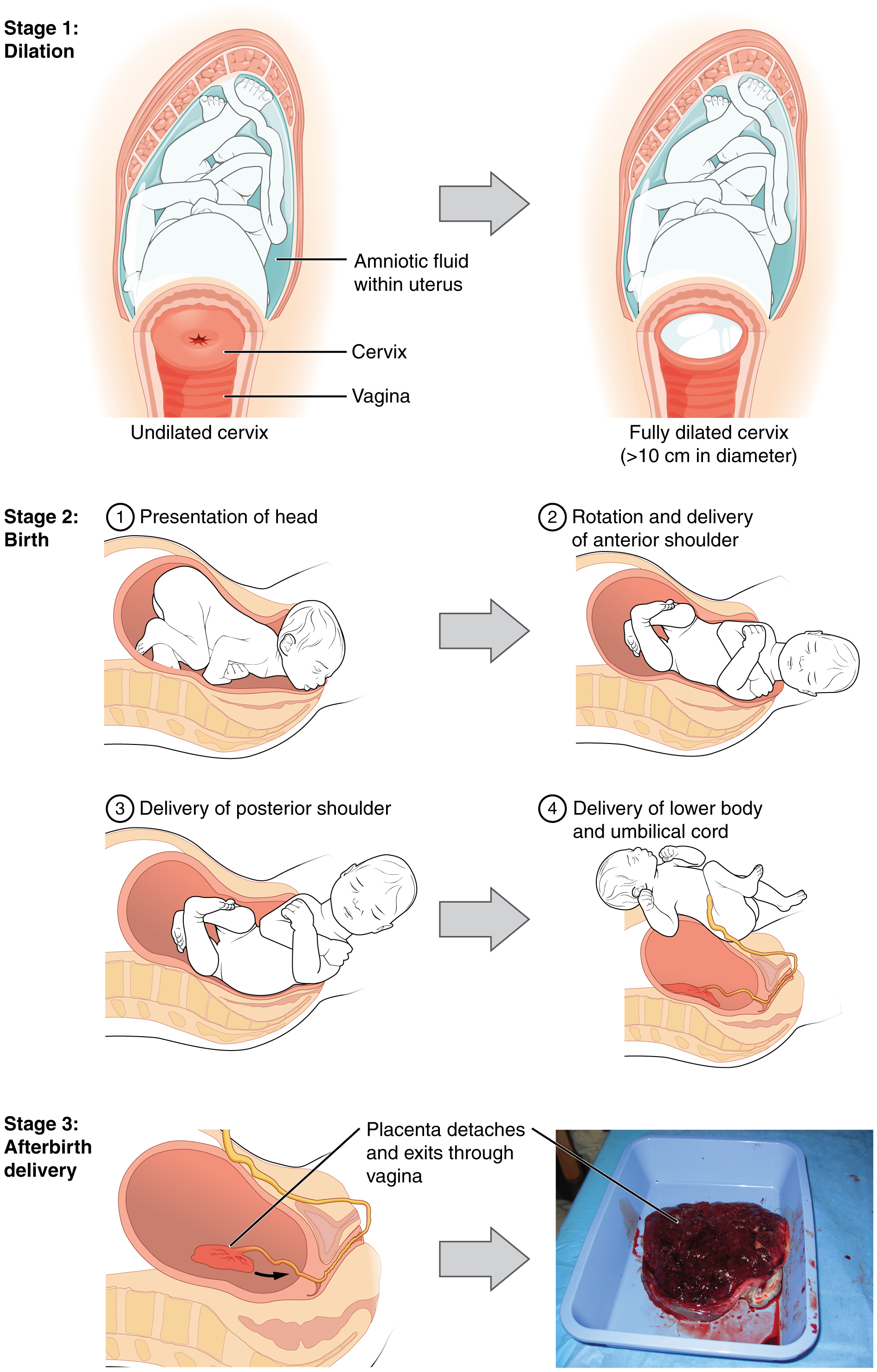
Near the time of birth, the amniotic sac — a fluid-filled membrane that encloses the fetus within the uterus — breaks in a gush of fluid. This is commonly called “breaking water.” Labor usually begins within a day of this event, although it may begin prior to it. Labor is the general term for the process of childbirth in which regular uterine contractions push the fetus and placenta out of the body. Labor can be divided into three stages, which are illustrated in Figure \(\PageIndex{5}\): dilation, birth, and after birth.
- During the dilation stage of labor, uterine contractions begin and become increasingly frequent and intense. The contractions push the baby’s head (most often) against the cervix, causing the cervical canal to dilate, or become wider. This lasts until the cervical canal has dilated to about 10 cm (3.9 in.) in width, which may take 12 to 20 hours — or even longer. The cervical canal must be dilated to this extent in order for the baby’s head to fit through it.
- During birth, the baby descends (usually headfirst) through the cervical canal and vagina, and into the world outside. This is the stage when the mother generally starts bearing down during the contractions to help push out the fetus. The fetus exits the vagina with its face facing the mother's posterior. It takes a 90-degree turn as the shoulders are delivered. This stage may last from about 20 minutes to two hours or more. Usually, within a minute or less of birth, the umbilical cord is cut, so the baby is no longer connected to the placenta.
- During the afterbirth stage, the placenta is delivered. This stage may last from a few minutes to a half hour.
Delivery is a matter of concern for all individuals. However, additional concerns arise for individuals with disabilities. According to a study done by Lipson and Rogers, delivery decisions for disabled individuals are made arbitrarily without their consent. They are forced to deliver via cesarean section because they think that a disabled person wouldn't be able to handle the process.
There are many myths associated with pregnancy. Most are harmless, but some may put the pregnant woman or fetus at risk. As always, knowledge is power.
Myth: You should avoid petting your cat during pregnancy.
Reality: Cat feces may be contaminated with microscopic parasites that can cause a disease called toxoplasmosis. Pregnant women who contract this disease are at risk of stillbirth, miscarriage, or giving birth to an infant with serious health problems. Pregnant women should not have contact with a cat’s litter box or feces, but petting a cat poses no real risk of infection.
Myth: You should not dye your hair during pregnancy, because the chemicals can harm the fetus.
Reality: Whereas some chemicals (such as certain pesticides) have been shown to be associated with birth defects, there is no evidence that using hair dye during pregnancy increases this risk.
Myth: A pregnant woman needs to eat for two, so she should double her pre-pregnancy caloric intake.
Reality: Throughout a typical pregnancy, a person needs only about 300 extra calories per day, on average, to support her growing fetus. Most of the extra calories are needed during the last trimester when the fetus is growing most rapidly. Doubling her caloric intake during pregnancy is likely to cause too much weight gain, which can be detrimental to her baby. Babies that weigh much more than the average 7.5 pounds at birth are more likely to develop diabetes and obesity in later life.
Myth: Women who are pregnant have strange food cravings, such as ice cream with pickles.
Reality: Some women do have food cravings during pregnancy, but they are not necessarily cravings for strange foods or unusual food combinations. For example, a pregnant woman might crave starchy foods for a few weeks, or she may be put off by certain foods that she loved before pregnancy.
Myth: A pregnant woman has skin that glows.
Reality: Pregnancy can actually be hard on the skin and its appearance. Besides stretch marks on the abdomen and breasts, pregnancy may lead to spider veins, varicose veins, new freckles, darkening of moles, and acne flare-ups. In addition, as many as 75 percent of pregnant women experience chloasma, which is the emergence of blotchy brown patches of skin on the face due to high estrogen levels. Chloasma is often referred to as the “mask of pregnancy.”
Myth: Men cannot carry a baby.
Reality: Transgender men can get pregnant using alternative methods.
Review
1. What is oogenesis? How does it occur?
2. Describe the maturation of an ovarian follicle.
3. Define ovulation.
4. What is happening in the uterus while a follicle in the ovary is maturing?
5. After a secondary oocyte is ovulated from the ovary, it may or may not be fertilized. Contrast what happens next in each of these different outcomes.
6. What is pregnancy, and what is the role of the maternal organism in pregnancy?
7. What is the average duration of pregnancy? Identify the trimesters of pregnancy.
8. Define labor. What event is often a sign that labor will soon begin?
9. Identify the stages of labor.
10. Describe the physiological function of female breasts. How is this function controlled?
11. Identify the functions of the female sex hormones estrogen and progesterone.
12. True or False: All of the developing gametes in an ovary complete meiosis I at the time of puberty.
13. True or False: After fertilization, meiosis II is completed, and then mitosis occurs.
14. A fertilized egg that has not yet implanted in the uterus is called a(n) ________________.
A. embryo
B. zygote
C. fetus
D. secondary oocyte
15. Describe the roles of the cervix in fertilization and childbirth.
Explore More
Attributions
- Pregnant woman by Øyvind Holmstad, CC BY-SA 4.0 via Wikimedia Commons
- Oogenesis by OpenStax College, CC BY 3.0 via Wikimedia Commons
- Fertilization by Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. licensed CC BY 3.0 via Wikimedia Commons
- Pregnancy comparison by Maustrauser, public domain via Wikimedia Commons
- Stages of labor by OpenStax College, CC BY 3.0 via Wikimedia Commons
- Text adapted from Human Biology by CK-12 licensed CC BY-NC 3.0
- Some text is adapted from Trautner, Emily et al. “Knowledge and practice of induction of lactation in trans women among professionals working in trans health.” International breastfeeding journal vol. 15,1 63. 16 Jul. 2020, doi:10.1186/s13006-020-00308-6; CC BY 4.0