
4.6: Contraception
- Page ID
- 187724

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Marie Stopes was a British author and paleobotanist (1880 to 1958) who made significant contributions to science and was the first woman on the faculty of the University of Manchester in England. Her most lasting impact is the work she did as a family-planning pioneer.
Stopes founded the first birth control clinic in Britain, along with her husband. She edited a newsletter called Birth Control News, which gave explicit, practical advice on how to avoid unwanted pregnancies, and in 1918, published a sex manual titled Married Love. The book was controversial and influential, bringing the subject of contraception into wide public discourse for the first time.

Figure \(\PageIndex{1}\): Marie Stopes in her laboratory in 1904. Unknown CC0.
Unintended Pregnancy
An unintended pregnancy is a pregnancy that is either mistimed or unwanted at the time of conception. It is a core concept in understanding the fertility of populations and the unmet need for contraception. Unintended pregnancy is associated with an increased risk of morbidity for women and with unhealthy behaviors during pregnancy. For example, women with an unintended pregnancy may delay prenatal care, which may affect the health of the infant. Women of all ages may have unintended pregnancies, but some groups, such as teens, are at a higher risk.
Efforts to decrease unintended pregnancy include finding better forms of contraception and increasing contraceptive use and adherence.
What is Contraception?
About a century after Married Love, more than half of all fertile married couples worldwide use some form of contraception. Contraception, also known as birth control, is any method or device used to prevent pregnancy. Birth control methods have been used for centuries, but safe and effective methods only became available in the 20th century, in part because of the work of people like Marie Stopes.
Many different birth control methods are currently available, but they differ considerably in their effectiveness at preventing pregnancy. The effectiveness of contraception is generally expressed as the failure rate, which is the percentage of women who become pregnant using a given method during the first year of use. Virtually no one uses any method of birth control perfectly, so the failure rate with typical use is almost always higher — and often much higher — than the failure rate with perfect use.
For example, with perfect use, a birth control method might have a failure rate of just one percent, whereas, with typical use, the failure rate might be 25 percent. For comparison, there is an average 85% chance of pregnancy in one year if no contraception is used with heterosexual sex.
All methods of birth control have potential adverse effects, but their health risks are less than the health risks associated with pregnancy. Using contraception to space children is good for the mother's health, the children’s health, and their development.
The choice of birth control depends on factors such as a person’s overall health, age, frequency of sexual activity, number of sexual partners, desire to have children in the future, and family history of certain diseases. A woman should talk to her health care provider about her choice of birth control method.
It is important to remember that even though birth control methods can prevent pregnancy, they do not all protect against sexually transmitted infections (STIs), including HIV.
Types of Contraception and Their Effectiveness
Types of birth control methods include barrier methods, hormonal methods, intrauterine devices, behavioral methods, and sterilization. With the exception of sterilization, all of these methods are reversible. Examples of each type of birth control method and their failure rates with typical adherence are described below.
Barrier Methods
Barrier methods, including male and female condoms and diaphragms, are devices that are used to physically block sperm from entering the uterus. They include condoms and diaphragms. There is an 18% chance of pregnancy using this method with typical adherence.
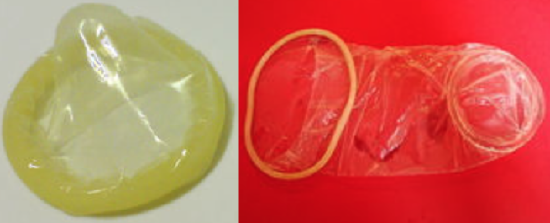
Condoms
Condoms are the most commonly used method of birth control globally. Condoms work by physically blocking sperm from entering the vagina of the sexual partner. There are condoms for vaginas and penises, but penis condoms are more widely used, less expensive, and more readily available. Both types of condoms are pictured in Figure \(\PageIndex{2}\). With typical use, penis condoms have an 18% failure rate, and vagina condoms have a 21% failure rate.
Condoms protect against and prevent the spread of many STIs, unlike virtually all other birth control methods.
Regardless of whether a condom for the vagina or penis is used, it must be put in place before sexual intercourse to protect against STIs and prevent pregnancy, since some sperm are released prior to ejaculation.
Diaphragms
Diaphragms, like the one in Figure \(\PageIndex{3}\), ideally prevent sperm from passing through the cervical canal and into the uterus. A diaphragm is inserted vaginally before sexual intercourse and must be placed over the cervix to be effective. It is usually recommended to cover a diaphragm with spermicide before insertion for extra protection. It is also recommended to leave the diaphragm in place for at least six hours after intercourse.
The failure rate of diaphragms with typical use is about 12%, which is about half that of condoms. However, diaphragms do not help prevent the spread of STIs, and their use is also associated with an increased frequency of urinary tract infections.
Diaphragms do not protect against STIs.

Hormonal Methods
Hormonal contraception is the administration of hormones to prevent ovulation. Hormones can be taken orally in birth control pills, implanted under the skin, injected into a muscle, or received transdermally from a skin patch.
Hormonal methods are currently available only for individuals with a uterus and ovaries. Birth control pills are the most common form of hormonal contraception. There are two types of pills: the combined pill (which contains both estrogen and progesterone) and the progesterone-only pill. Both types of pills inhibit ovulation and thicken cervical mucus.
The failure rate of birth control pills is less than 1% if used perfectly. The pregnancy rate with this method is 6-12% based on actual use, largely because individuals do not always remember to take the pill at the same time every day to maintain a steady level of hormone(s).
The combined pill is associated with a slightly increased risk of blood clots, but a reduced risk of ovarian and endometrial cancers. The progesterone-only pill does not increase the risk of blood clots, but it may cause irregular menstrual periods. It may take a few weeks or months for fertility to return to normal after the long-term use of birth control pills.
Hormonal contraception does not protect against STIs.
Intrauterine Devices
An intrauterine device (IUD) is a T-shaped or coiled plastic structure that is inserted into the uterus via the vagina and cervix and contains either copper or a hormone (Figure \(\PageIndex{4}\)). An IUD is inserted by a physician and may be left in place for months or even years. A physician must also remove an IUD using the device's strings.
The failure rates for both types of IUDs below are less than 1%, leading to their wide use. Once an IUD is removed, even after long-term use, fertility usually immediately returns to normal.
IUDs do have complication risks: increased menstrual bleeding, more painful menstrual cramps, the possibility of being expelled from the uterus, and a slight risk of perforation of the uterus.
IUDs do not protect against STIs.
Copper IUDs
The copper in copper IUDs prevents pregnancy by interfering with the movement of sperm so they cannot reach and fertilize an egg. The copper may also prevent implantation in the unlikely event that a sperm manages to reach and fertilize an egg. The failure rate with this method is less than 1%.
Hormonal IUDs
Hormonal IUDs prevent pregnancy by thickening cervical mucus and trapping sperm. The hormones may also interfere with ovulation, so no egg is available to be fertilized.
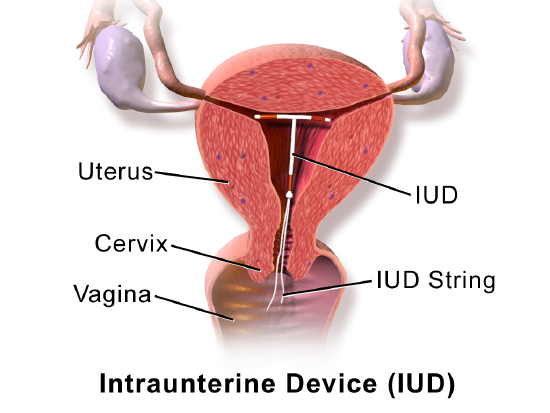
Figure \(\PageIndex{4}\): An IUD is a T-shaped structure. two ends of the IUD block the openings of the two fallopian tubes and the third end contains IUD string that hangs out of the cervix into the vagina. Intrauterine Device (IUD). Medical gallery of Blausen Medical 2014 CC-BY 3.0
Sterilization
The most effective contraceptive method is sterilization. In both sexes, sterilization generally involves surgical procedures that are considered irreversible. Male sterilization is less invasive and less risky than female sterilization.
Additional surgery may be able to reverse a sterilization procedure, but there are no guarantees.
Sterilization does not protect against STIs.
Male Sterilization
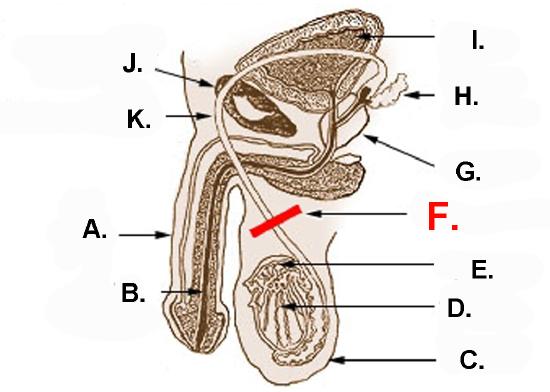
Male sterilization is usually achieved with a vasectomy. In this surgery, the vas deferens from each testis is clamped, cut, or otherwise sealed (Figure \(\PageIndex{6}\)). This prevents sperm from traveling from the epididymis to the ejaculatory ducts and being ejaculated from the penis.
The same amount of semen will still be ejaculated, but it will not contain any sperm, making fertilization impossible. After a vasectomy, the testes continue to produce sperm, but the sperm are reabsorbed.
It usually takes several months after a vasectomy for all remaining sperm to be ejaculated or reabsorbed. In the meantime, another method of birth control should be used.
Female Sterilization
The procedure undertaken for female sterilization is usually tubal ligation. The Fallopian tubes may be tied or cut in a surgical procedure, which permanently blocks the tubes. Alternatively, tiny metal implants may be inserted into the Fallopian tubes in a nonsurgical procedure. Over time, scar tissue forms around the implants, permanently blocking the tubes. Either method prevents eggs from traveling from the ovaries through the Fallopian tubes, where fertilization usually occurs.
Behavioral Methods
The least effective methods of contraception are behavioral methods. They involve regulating the timing or method of intercourse to prevent the introduction of sperm into the uterus, either altogether or when an egg may be present. Behavioral methods include fertility awareness methods and withdrawal.
Behavioral methods, other than total abstinence, do not protect against STIs.
Abstinence
Abstinence means abstaining from vaginal, anal, or oral sexual activity at any time. This method is 100% effective in preventing pregnancy and protecting against STIs.
Some may use a modified form of abstinence by abstaining from vaginal intercourse to avoid pregnancy. This method is not effective in protecting against STIs unless paired with condoms and/or a dental dam.
Abstinence is sometimes considered a behavioral method, but it is unlikely to be practiced consistently enough by most people to prevent pregnancy.
Abstinence-only sex education does not lead to reduced rates of pregnancy.
Withdrawal
Withdrawal (also called coitus interruptus) is the practice of withdrawing the penis from the vagina before ejaculation occurs. The withdrawal method has a high failure rate 22% with typical use. The main risks of the withdrawal method include:
- the penis is not withdrawn in a timely manner.
- some sperm are released from the penis before ejaculation occurs.
- if sperm are ejaculated just outside of the vagina, there is a chance they will be able to enter the vagina and travel up to fertilize an egg.
Fertility Awareness Methods
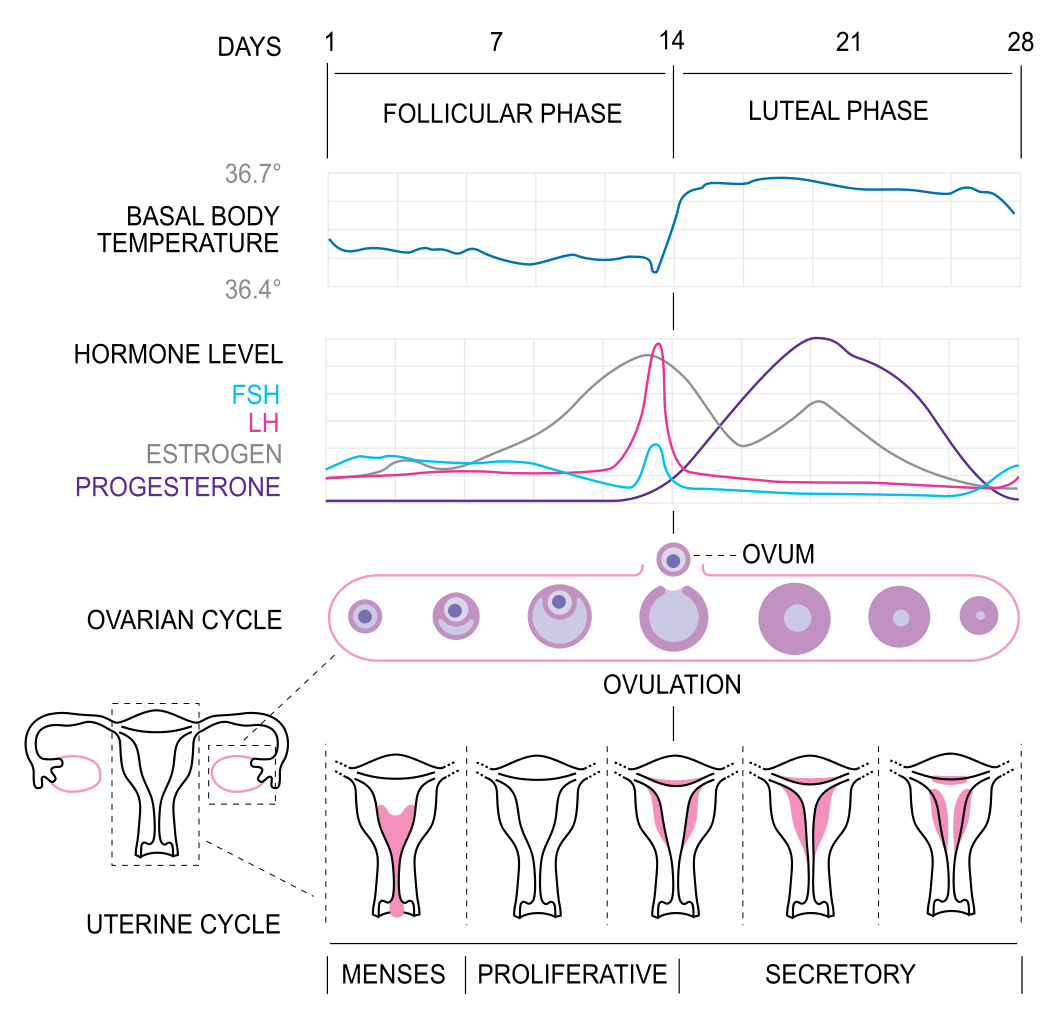
Fertility awareness methods involve estimating the most fertile days of the menstrual cycle and then avoiding unprotected vaginal intercourse on those days. The most fertile days are generally a few days before ovulation occurs, the day of ovulation, and another day or two after that. Sperm can live for up to a week in the female reproductive tract, so determining the occurrence of ovulation only after the fact is a major drawback of this method.
Unless unprotected sex occurs on those days, pregnancy is unlikely. Techniques for estimating the most fertile days include monitoring and detecting minor changes in basal body temperature or cervical secretions. Using this method requires a regular menstrual cycle, motivation, and diligence, so typical-use failure rates can exceed 25%. Some individuals may experience failure rates as high as 85%, the same as using no contraception at all.
Emergency Contraception (EC)
Emergency contraception is any form of contraception that is used after unprotected vaginal intercourse. This may be due to the failure of a contraceptive device (e.g., a condom breaks), a missed dose of a hormone contraceptive, unplanned intercourse, or sexual assault. If taken within 24 hours of unprotected vaginal intercourse, emergency contraception has an average failure rate of less than 5%.
Emergency contraception does not prevent STIs.
Hormonal EC
Also known as the “morning-after” pill, hormonal ECs are high-dose birth control pills that help prevent pregnancy by delaying or inhibiting ovulation. It works only if ovulation has not already occurred, only if a pregnancy has not been established, and only when taken within five days after unprotected sex. EC pills do not cause an abortion.
Some hormonal ECs are available over the counter, and others only by prescription. The sooner the pill is taken, the more likely it is to work.
In a 2021 study, researchers asked over 500 participants to explain how the morning-after pill worked. Despite these pills’ widespread use, 60% answered incorrectly. Emergency contraceptives are often misunderstood— even the phrase “the morning-after pill” is a misnomer. So, how do they work? Alison Edelman explores how two main types of emergency contraception disrupt or delay ovulation.
IUD EC
Another method of emergency contraception is the IUD. An IUD that is inserted up to five days after unprotected sex can prevent nearly 100 percent of pregnancies.
Emergency IUDs keep sperm from reaching and fertilizing an egg or inhibit implantation if an egg has already been fertilized. The IUD can then be left in place to prevent future pregnancies.
IUD ECs are only available by visiting a doctor or clinic.
Sexual Assault Resources
If you, a friend, or other loved one has been sexually assaulted, please use the following resources to help guide you and provide additional resources:
- Your campus's Student Service resources
- RAINN National Sexual Assault Hotline