
4.10: Helminthic Infections of the Gastrointestinal Tract
- Page ID
- 79544

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Learning Objectives
- Identify the most common helminths that cause infections of the GI tract
- Compare the major characteristics of specific helminthic diseases affecting GI tract
Helminths are widespread intestinal parasites. These parasites can be divided into three common groups: round-bodied worms also described as nematodes, flat-bodied worms that are segmented (also described as cestodes), and flat-bodied worms that are non-segmented (also described as trematodes). The nematodes include roundworms, pinworms, hookworms, and whipworms. Cestodes include beef, pork, and fish tapeworms. Trematodes are collectively called flukes and more uniquely identified with the body site where the adult flukes are located. Although infection can have serious consequences, many of these parasites are so well adapted to the human host that there is little obvious disease.
Ascariasis
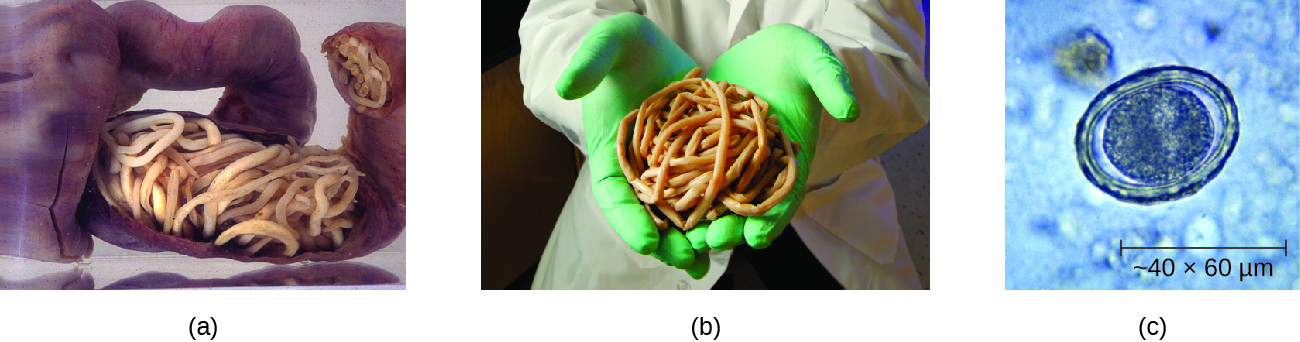
Infections caused by the large nematode roundworm Ascaris lumbricoides, a soil-transmitted helminth, are called ascariasis. Over 800 million to 1 billion people are estimated to be infected worldwide.1 Infections are most common in warmer climates and at warmer times of year. At present, infections are uncommon in the United States. The eggs of the worms are transmitted through contaminated food and water. This may happen if food is grown in contaminated soil, including when manure is used as fertilizer.
When an individual consumes embryonated eggs (those with a developing embryo), the eggs travel to the intestine and the larvae are able to hatch. Ascaris is able to produce proteases that allow for penetration and degradation of host tissue. The juvenile worms can then enter the circulatory system and migrate to the lungs where they enter the alveoli (air sacs). From here they crawl to the pharynx and then follow the gut lumen to return to the small intestine, where they mature into adult roundworms. Females in the host will produce and release eggs that leave the host via feces. In some cases, the worms can block ducts such as those of the pancreas or gallbladder.
The infection is commonly asymptomatic. When signs and symptoms are present, they include shortness of breath, cough, nausea, diarrhea, blood in the stool, abdominal pain, weight loss, and fatigue. The roundworms may be visible in the stool. In severe cases, children with substantial infections may experience intestinal blockage.
The eggs can be identified by microscopic examination of the stool (Figure \(\PageIndex{1}\)). In some cases, the worms themselves may be identified if coughed up or excreted in stool. They can also sometimes be identified by X-rays, ultrasounds, or MRIs.
Ascariasis is self-limiting, but can last one to two years because the worms can inhibit the body’s inflammatory response through glycan gimmickry (see Virulence Factors of Eukaryotic Pathogens). The first line of treatment is mebendazole or albendazole. In some severe cases, surgery may be required.
Exercise \(\PageIndex{1}\)
Describe the route by which A. lumbricoides reaches the host’s intestines as an adult worm.
Hookworm
Two species of nematode worms are associated with hookworm infection. Both species are found in the Americas, Africa, and Asia. Necator americanus is found predominantly in the United States and Australia. Another species, Ancylostoma doudenale, is found in southern Europe, North Africa, the Middle East, and Asia. The eggs of these species develop into larvae in soil contaminated by dog or cat feces. These larvae can penetrate the skin. After traveling through the venous circulation, they reach the lungs. When they are coughed up, they are then swallowed and can enter the intestine and develop into mature adults. At this stage, they attach to the wall of the intestine, where they feed on blood and can potentially cause anemia. Signs and symptoms include cough, an itchy rash, loss of appetite, abdominal pain, and diarrhea. In children, hookworms can affect physical and cognitive growth.
Some hookworm species, such as Ancylostoma braziliense that is commonly found in animals such as cats and dogs, can penetrate human skin and migrate, causing cutaneous larva migrans, a skin disease caused by the larvae of hookworms. As they move across the skin, in the subcutaneous tissue, pruritic tracks appear (Figure \(\PageIndex{2}\)).
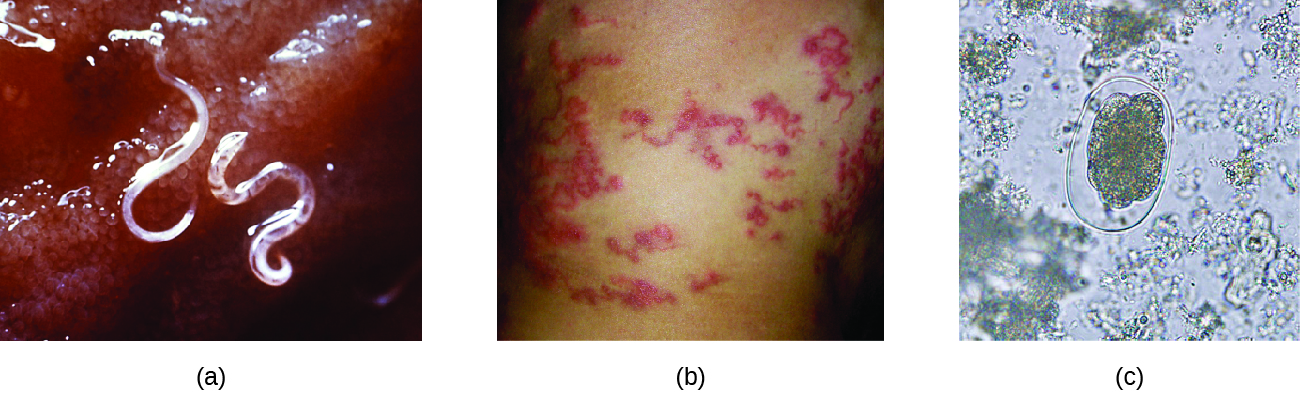
The infection is diagnosed using microscopic examination of the stool, allowing for observation of eggs in the feces. Medications such as albendazole, mebendazole, and pyrantel pamoate are used as needed to treat systemic infection. In addition to systemic medication for symptoms associated with cutaneous larva migrans, topical thiabendazole is applied to the affected areas.
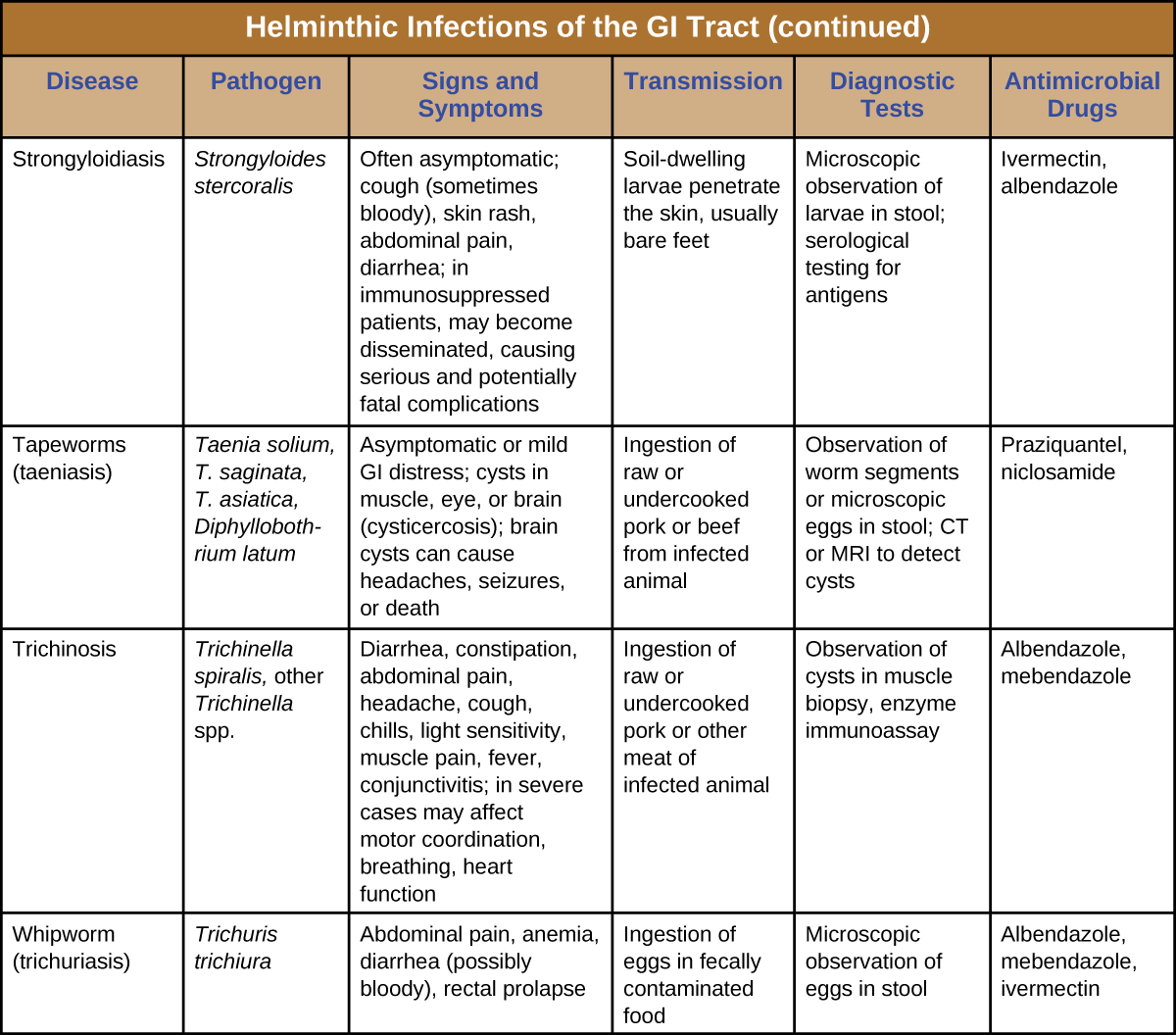
Strongyloidiasis
Strongyloidiasis is generally caused by Strongyloides stercoralis, a soil-transmitted helminth with both free-living and parasitic forms. In the parasitic form, the larvae of these nematodes generally penetrate the body through the skin, especially through bare feet, although transmission through organ transplantation or at facilities like day-care centers can also occur. When excreted in the stool, larvae can become free-living adults rather than developing into the parasitic form. These free-living worms reproduce, laying eggs that hatch into larvae that can develop into the parasitic form. In the parasitic life cycle, infective larvae enter the skin, generally through the feet. The larvae reach the circulatory system, which allows them to travel to the alveolar spaces of the lungs. They are transported to the pharynx where, like many other helminths, the infected patient coughs them up and swallows them again so that they return to the intestine. Once they reach the intestine, females live in the epithelium and produce eggs that develop asexually, unlike the free-living forms, which use sexual reproduction. The larvae may be excreted in the stool or can reinfect the host by entering the tissue of the intestines and skin around the anus, which can lead to chronic infections.
The condition is generally asymptomatic, although severe symptoms can develop after treatment with corticosteroids for asthma or chronic obstructive pulmonary disease, or following other forms of immunosuppression. When the immune system is suppressed, the rate of autoinfection increases, and huge amounts of larvae migrate to organs throughout the body.
Signs and symptoms are generally nonspecific. The condition can cause a rash at the site of skin entry, cough (dry or with blood), fever, nausea, difficulty breathing, bloating, pain, heartburn, and, rarely, arthritis, or cardiac or kidney complications. Disseminated strongyloidiasis or hyperinfection is a life-threatening form of the disease that can occur, usually following immunosuppression such as that caused by glucocorticoid treatment (most commonly), with other immunosuppressive medications, with HIV infection, or with malnutrition.
As with other helminths, direct examination of the stool is important in diagnosis. Ideally, this should be continued over seven days. Serological testing, including antigen testing, is also available. These can be limited by cross-reactions with other similar parasites and by the inability to distinguish current from resolved infection. Ivermectin is the preferred treatment, with albendazole as a secondary option.
Exercise \(\PageIndex{2}\)
How does an acute infection of S. stercoralis become chronic?
Pinworms (Enterobiasis)
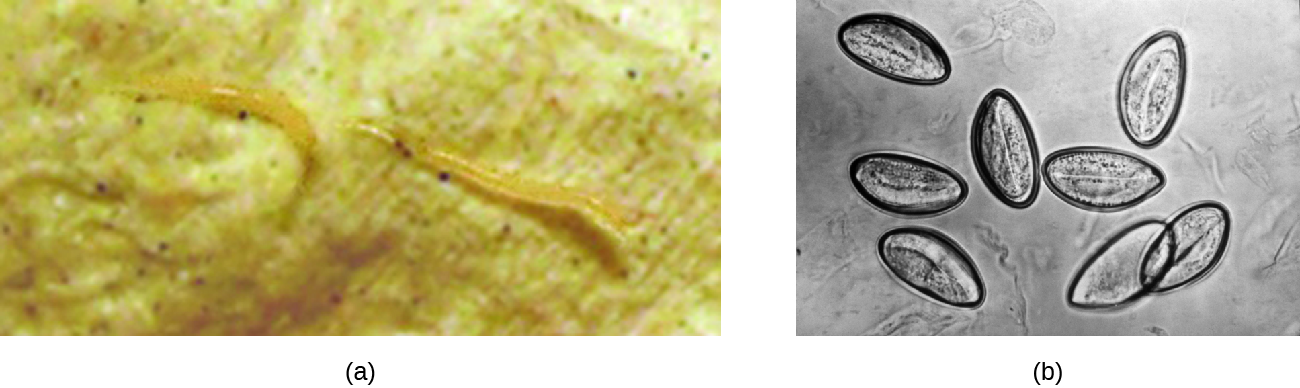
Enterobius vermicularis, commonly called pinworms, are tiny (2–13 mm) nematodes that cause enterobiasis. Of all helminthic infections, enterobiasis is the most common in the United States, affecting as many as one-third of American children.2 Although the signs and symptoms are generally mild, patients may experience abdominal pain and insomnia from itching of the perianal region, which frequently occurs at night when worms leave the anus to lay eggs. The itching contributes to transmission, as the disease is transmitted through the fecal-oral route. When an infected individual scratches the anal area, eggs may get under the fingernails and later be deposited near the individual’s mouth, causing reinfection, or on fomites, where they can be transferred to new hosts. After being ingested, the larvae hatch within the small intestine and then take up residence in the colon and develop into adults. From the colon, the female adult exits the body at night to lay eggs (Figure \(\PageIndex{3}\)).
Infection is diagnosed in any of three ways. First, because the worms emerge at night to lay eggs, it is possible to inspect the perianal region for worms while an individual is asleep. An alternative is to use transparent tape to remove eggs from the area around the anus first thing in the morning for three days to yield eggs for microscopic examination. Finally, it may be possible to detect eggs through examination of samples from under the fingernails, where eggs may lodge due to scratching. Once diagnosis has been made, mebendazole, albendazole, and pyrantel pamoate are effective for treatment.
Trichuriasis
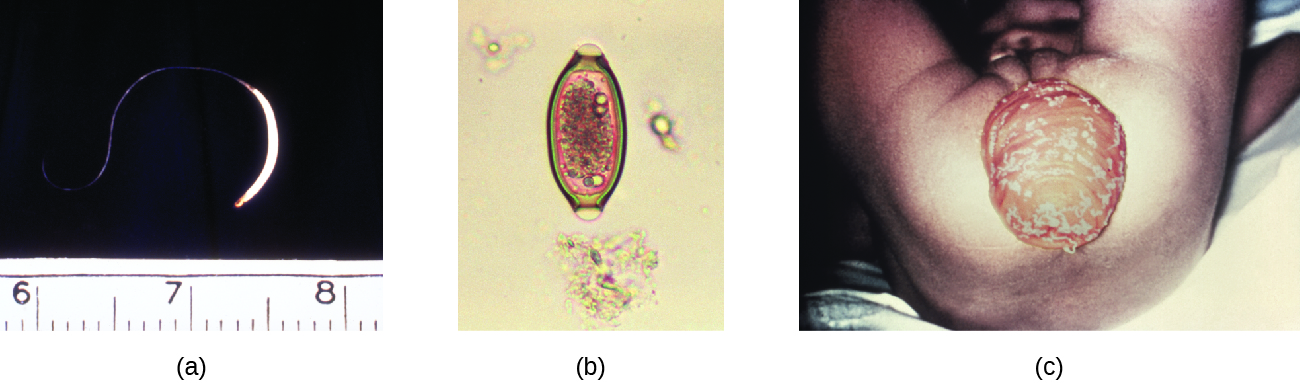
The nematode whipworm Trichuris trichiura is a parasite that is transmitted by ingestion from soil-contaminated hands or food and causes trichuriasis. Infection is most common in warm environments, especially when there is poor sanitation and greater risk of fecal contamination of soil, or when food is grown in soil using manure as a fertilizer. The signs and symptoms may be minimal or nonexistent. When a substantial infection develops, signs and symptoms include painful, frequent diarrhea that may contain mucus and blood. It is possible for the infection to cause rectal prolapse, a condition in which a portion of the rectum becomes detached from the inside of the body and protrudes from the anus (Figure \(\PageIndex{4}\)). Severely infected children may experience reduced growth and their cognitive development may be affected.
When fertilized eggs are ingested, they travel to the intestine and the larvae emerge, taking up residence in the walls of the colon and cecum. They attach themselves with part of their bodies embedded in the mucosa. The larvae mature and live in the cecum and ascending colon. After 60 to 70 days, females begin to lay 3000 to 20,000 eggs per day.
Diagnosis involves examination of the feces for the presence of eggs. It may be necessary to use concentration techniques and to collect specimens on multiple days. Following diagnosis, the infection may be treated with mebendazole, albendazole, or ivermectin.
Trichinosis
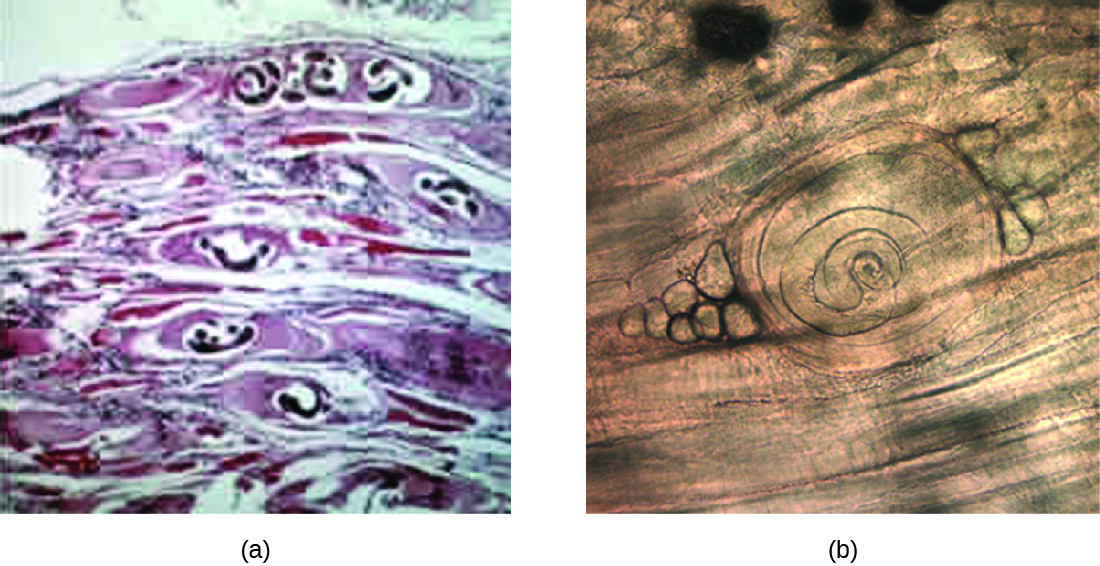
Trichinosis (trichenellosis) develops following consumption of food that contains Trichinella spiralis (most commonly) or other Trichinella species. These microscopic nematode worms are most commonly transmitted in meat, especially pork, that has not been cooked thoroughly. T. spiralis larvae in meat emerge from cysts when exposed to acid and pepsin in the stomach. They develop into mature adults within the large intestine. The larvae produced in the large intestine are able to migrate into the muscles mechanically via the stylet of the parasite, forming cysts. Muscle proteins are reduced in abundance or undetectable in cells that contain Trichinella (nurse cells). Animals that ingest the cysts from other animals can later develop infection (Figure \(\PageIndex{5}\)).
Although infection may be asymptomatic, symptomatic infections begin within a day or two of consuming the nematodes. Abdominal symptoms arise first and can include diarrhea, constipation, and abdominal pain. Other possible symptoms include headache, light sensitivity, muscle pain, fever, cough, chills, and conjunctivitis. More severe symptoms affecting motor coordination, breathing, and the heart sometimes occur. It may take months for the symptoms to resolve, and the condition is occasionally fatal. Mild cases may be mistaken for influenza or similar conditions.
Infection is diagnosed using clinical history, muscle biopsy to look for larvae, and serological testing, including immunoassays. Enzyme immunoassay is the most common test. It is difficult to effectively treat larvae that have formed cysts in the muscle, although medications may help. It is best to begin treatment as soon as possible because medications such as mebendazole and albendazole are effective in killing only the adult worms in the intestine. Steroids may be used to reduce inflammation if larvae are in the muscles.
Exercise \(\PageIndex{3}\)
Compare and contrast the transmissions of pinworms and whipworms.
Tapeworms (Taeniasis)
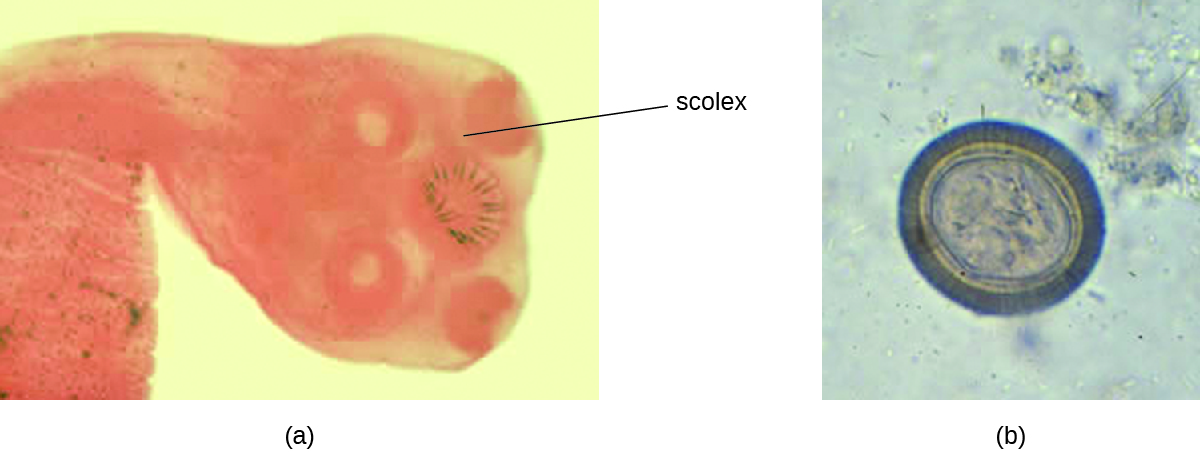
Taeniasis is a tapeworm infection, generally caused by pork (Taenia solium), beef (Taenia saginata), and Asian (Taenia asiatica) tapeworms found in undercooked meat. Consumption of raw or undercooked fish, including contaminated sushi, can also result in infection from the fish tapeworm (Diphyllobothrium latum). Tapeworms are flatworms (cestodes) with multiple body segments and a head called a scolex that attaches to the intestinal wall. Tapeworms can become quite large, reaching 4 to 8 meters long (Figure \(\PageIndex{6}\)). Figure 5.2.5 illustrates the life cycle of a tapeworm.
Tapeworms attached to the intestinal wall produce eggs that are excreted in feces. After ingestion by animals, the eggs hatch and the larvae emerge. They may take up residence in the intestine, but can sometimes move to other tissues, especially muscle or brain tissue. When T. solium larvae form cysts in tissue, the condition is called cysticercosis. This occurs through ingestion of eggs via the fecal-oral route, not through consumption of undercooked meat. It can develop in the muscles, eye (ophthalmic cysticercosis), or brain (neurocysticercosis).
Infections may be asymptomatic or they may cause mild gastrointestinal symptoms such as epigastric discomfort, nausea, diarrhea, flatulence, or hunger pains. It is also common to find visible tapeworm segments passed in the stool. In cases of cysticercosis, symptoms differ depending upon where the cysts become established. Neurocysticercosis can have severe, life-threatening consequences and is associated with headaches and seizures because of the presence of the tapeworm larvae encysted in the brain. Cysts in muscles may be asymptomatic, or they may be painful.
To diagnose these conditions, microscopic analysis of stool samples from three separate days is generally recommended. Eggs or body segments, called proglottids, may be visible in these samples. Molecular methods have been developed but are not yet widely available. Imaging, such as CT and MRI, may be used to detect cysts. Praziquantel or niclosamide are used for treatment.
What’s in Your Sushi Roll?
As foods that contain raw fish, such as sushi and sashimi, continue to increase in popularity throughout the world, so does the risk of parasitic infections carried by raw or undercooked fish. Diphyllobothrium species, known as fish tapeworms, is one of the main culprits. Evidence suggests that undercooked salmon caused an increase in Diphyllobothrium infections in British Columbia in the 1970s and early 1980s. In the years since, the number of reported cases in the United States and Canada has been low, but it is likely that cases are underreported because the causative agent is not easily recognized.3
Another illness transmitted in undercooked fish is herring worm disease, or anisakiasis, in which nematodes attach to the epithelium of the esophagus, stomach, or small intestine. Cases have increased around the world as raw fish consumption has increased.4
Although the message may be unpopular with sushi lovers, fish should be frozen or cooked before eating. The extremely low and high temperatures associated with freezing and cooking kill worms and larvae contained in the meat, thereby preventing infection. Ingesting fresh, raw sushi may make for a delightful meal, but it also entails some risk.
Hydatid Disease
Another cestode, Echinococcus granulosus, causes a serious infection known as hydatid disease (cystic echinococcosis). E. granulosus is found in dogs (the definitive host), as well as several intermediate hosts (sheep, pigs, goats, cattle). The cestodes are transmitted through eggs in the feces from infected animals, which can be an occupational hazard for individuals who work in agriculture.
Once ingested, E. granulosus eggs hatch in the small intestine and release the larvae. The larvae invade the intestinal wall to gain access to the circulatory system. They form hydatid cysts in internal organs, especially in the lungs and liver, that grow slowly and are often undetected until they become large. If the cysts burst, a severe allergic reaction (anaphylaxis) may occur.
Cysts present in the liver can cause enlargement of the liver, nausea, vomiting, right epigastric pain, pain in the right upper quadrant, and possible allergic signs and symptoms. Cysts in the lungs can lead to alveolar disease. Abdominal pain, weight loss, pain, and malaise may occur, and inflammatory processes develop.
E. granulosus can be detected through imaging (ultrasonography, CT, MRI) that shows the cysts. Serologic tests, including ELISA and indirect hemagglutinin tests, are used. Cystic disease is most effectively treated with surgery to remove cysts, but other treatments are also available, including chemotherapy with anti-helminthic drugs (albendazoleor mebendazole).
Exercise \(\PageIndex{4}\)
Describe the risks of the cysts associated with taeniasis and hydatid disease.
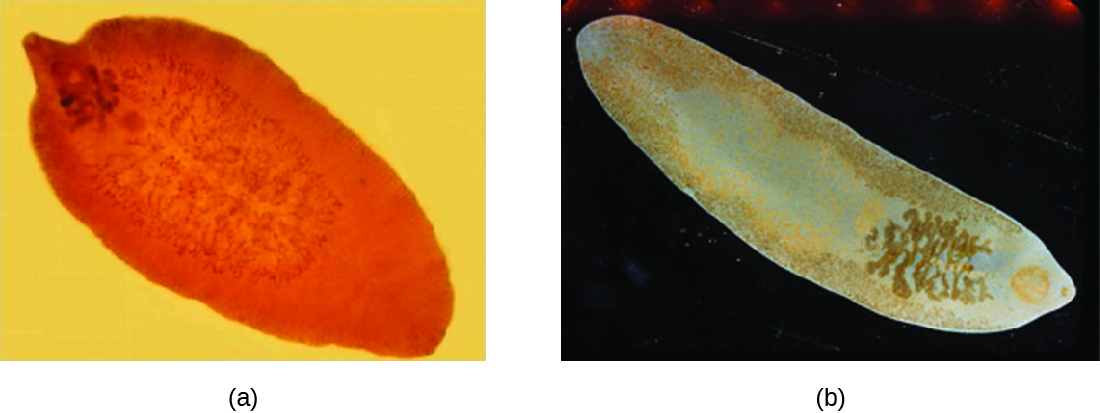
Flukes
Flukes are flatworms that have a leaflike appearance. They are a type of trematode worm, and multiple species are associated with disease in humans. The most common are liver flukes and intestinal flukes (Figure \(\PageIndex{7}\)).
Liver Flukes
The liver flukes are several species of trematodes that cause disease by interfering with the bile duct. Fascioliasis is caused by Fasciola hepatica and Fasciola gigantica in contaminated raw or undercooked aquatic plants (e.g., watercress). In Fasciola infection, adult flukes develop in the bile duct and release eggs into the feces. Clonochiasis is caused by Clonorchis sinensis in contaminated freshwater fish. Other flukes, such as Opisthorchis viverrini (found in fish) and Opisthorchis felineus (found in freshwater snails), also cause infections. Liver flukes spend part of their life cycle in freshwater snails, which serve as an intermediate host. Humans are typically infected after eating aquatic plants contaminated by the infective larvae after they have left the snail. Once they reach the human intestine, they migrate back to the bile duct, where they mature. The life cycle is similar for the other infectious liver flukes (see Figure 5.2.4).
When Fasciola flukes cause acute infection, signs and symptoms include nausea, vomiting, abdominal pain, rash, fever, malaise, and breathing difficulties. If the infection becomes chronic, with adult flukes living in the bile duct, then cholangitis, cirrhosis, pancreatitis, cholecystitis, and gallstones may develop. Symptoms are similar for infections by other liver flukes. Cholangiocarcinoma can occur from C. sinensis infection. The Opisthorchis species can also be associated with cancer development.
Diagnosis is accomplished using patient history and examination of samples from feces or other samples (such as vomitus). Because the eggs may appear similar, immunoassay techniques are available that can help distinguish species. The preferred treatment for fascioliasis is triclabendazole. C. sinensis and Opisthorchis spp. infections are treated with praziquantel or albendazole.
Intestinal Flukes
The intestinal flukes are trematodes that develop in the intestines. Many, such as Fasciolopsis buski, which causes fasciolopsiasis, are closely related to liver flukes. Intestinal flukes are ingested from contaminated aquatic plants that have not been properly cooked. When the cysts are consumed, the larvae emerge in the duodenum and develop into adults while attached to the intestinal epithelium. The eggs are released in stool.
Intestinal fluke infection is often asymptomatic, but some cases may involve mild diarrhea and abdominal pain. More severe symptoms such as vomiting, nausea, allergic reactions, and anemia can sometimes occur, and high parasite loads may sometimes lead to intestinal obstructions.
Diagnosis is the same as with liver flukes: examination of feces or other samples and immunoassay. Praziquantel is used to treat infections caused by intestinal flukes.
Exercise \(\PageIndex{5}\)
How are flukes transmitted?
Helminthic Gastrointestinal Infections
Numerous helminths are capable of colonizing the GI tract. Many such infections are asymptomatic, but others may cause signs and symptoms ranging from mild GI stress to severe systemic infection. Helminths have complex and unique life cycles that dictate their specific modes of transmission. Most helminthic infections can be treated with medications.
Key Concepts and Summary
- Helminths often cause intestinal infections after transmission to humans through exposure to contaminated soil, water, or food. Signs and symptoms are often mild, but severe complications may develop in some cases.
- Ascaris lumbricoides eggs are transmitted through contaminated food or water and hatch in the intestine. Juvenile larvae travel to the lungs and then to the pharynx, where they are swallowed and returned to the intestines to mature. These nematode roundworms cause ascariasis.
- Necator americanus and Ancylostoma doudenale cause hookworm infection when larvae penetrate the skin from soil contaminated by dog or cat feces. They travel to the lungs and are then swallowed to mature in the intestines.
- Strongyloides stercoralis are transmitted from soil through the skin to the lungs and then to the intestine where they cause strongyloidiasis.
- Enterobius vermicularis are nematode pinworms transmitted by the fecal-oral route. After ingestion, they travel to the colon where they cause enterobiasis.
- Trichuris trichiura can be transmitted through soil or fecal contamination and cause trichuriasis. After ingestion, the eggs travel to the intestine where the larvae emerge and mature, attaching to the walls of the colon and cecum.
- Trichinella spp. is transmitted through undercooked meat. Larvae in the meat emerge from cysts and mature in the large intestine. They can migrate to the muscles and form new cysts, causing trichinosis.
- Taenia spp. and Diphyllobothrium latum are tapeworms transmitted through undercooked food or the fecal-oral route. Taenia infections cause taeniasis. Tapeworms use their scolex to attach to the intestinal wall. Larvae may also move to muscle or brain tissue.
- Echinococcus granulosus is a cestode transmitted through eggs in the feces of infected animals, especially dogs. After ingestion, eggs hatch in the small intestine, and the larvae invade the intestinal wall and travel through the circulatory system to form dangerous cysts in internal organs, causing hydatid disease.
- Flukes are transmitted through aquatic plants or fish. Liver flukes cause disease by interfering with the bile duct. Intestinal flukes develop in the intestines, where they attach to the intestinal epithelium.
Footnotes
- 1 Centers for Disease Control and Prevention. “Parasites–Ascariasis.” Updated May 24, 2016. http://www.cdc.gov/parasites/ascariasis/index.html.
- 2 “Roundworms.” University of Maryland Medical Center Medical Reference Guide. Last reviewed December 9, 2014. https://umm.edu/health/medical/altme...ion/roundworms.
- 3 Nancy Craig. “Fish Tapeworm and Sushi.” Canadian Family Physician 58 (2012) 6: pp. 654–658. www.ncbi.nlm.nih.gov/pmc/articles/PMC3374688/.
- 4 Centers for Disease Control and Prevention. “Anisakiasis FAQs.” Updated November 12, 2012. http://www.cdc.gov/parasites/anisakiasis/faqs.html.
Contributors and Attributions
Nina Parker, (Shenandoah University), Mark Schneegurt (Wichita State University), Anh-Hue Thi Tu (Georgia Southwestern State University), Philip Lister (Central New Mexico Community College), and Brian M. Forster (Saint Joseph’s University) with many contributing authors. Original content via Openstax (CC BY 4.0; Access for free at https://openstax.org/books/microbiology/pages/1-introduction)