
14.7: Disorders of the Skeletal System
- Page ID
- 22550

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
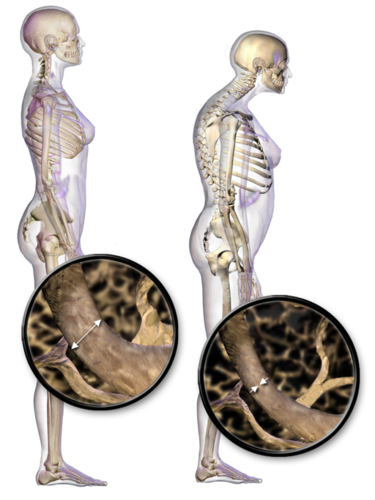
The individual on the right in Figure \(\PageIndex{1}\) has a deformity in her back commonly called dowager’s hump because it occurs most often in elderly women. Its medical name is kyphosis, and it is defined as excessive curvature of the spinal column in the thoracic region. The curvature generally results from fractures of thoracic vertebrae. As the inset drawings suggest, these fractures may occur due to a significant decrease in bone mass, which is called osteoporosis. Osteoporosis is one of the most prevalent disorders of the skeletal system.
Common Skeletal System Disorders
A number of disorders affect the skeletal system, including bone fractures and bone cancers. However, the two most common disorders of the skeletal system are osteoporosis and osteoarthritis. At least ten million people in the United States have osteoporosis, and more than 8 million of them are women. Osteoarthritis is even more common, affecting almost 30 million people in the United States. Because osteoporosis and osteoarthritis are so common, they are the focus of this concept. These two disorders are also good examples to illustrate the structure and function of the skeletal system.
Osteoporosis
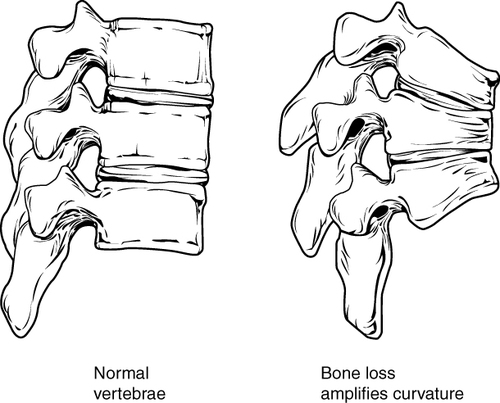
Osteoporosis is an age-related disorder in which bones lose mass, weaken, and break more easily than normal bones. Bones may weaken so much that a fracture can occur with minor stress — or even spontaneously, without any stress at all. Osteoporosis is the most common cause of broken bones in the elderly, but until a bone fracture occurs, it typically causes no symptoms. The bones that break most often include those in the wrist, hip, shoulder, and spine. When the thoracic vertebrae are affected, there can be a gradual collapse of the vertebrae due to compression fractures, as shown in Figure \(\PageIndex{2}\). This is what causes kyphosis, as pictured in Figure \(\PageIndex{1}\).
Changes in Bone Mass with Age
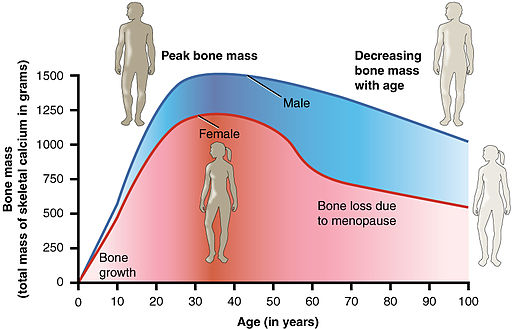
As shown in the graph below, bone mass in both males and females generally peaks when people are in their thirties. Bone mass usually decreases after that, and this tends to occur more rapidly in individuals with XX chromosomes, especially after menopause. This is generally attributable to low levels of estrogen in the post-menopausal years.
What Causes Osteoporosis?
Osteoporosis is due to an imbalance between bone formation by osteoblasts and bone resorption by osteoclasts. Normally, bones are constantly being remodeled by these two processes, with up to ten percent of all bone mass undergoing remodeling at any point in time. If these two processes are in balance, no net loss of bone occurs. There are three main ways that an imbalance between bone formation and bone resorption can occur and lead to a net loss of bone.
- An individual never develops normal peak bone mass during the young adult years: If the peak level is lower than normal, then there is less bone mass, to begin with, making osteoporosis more likely to develop.
- There is greater than normal bone resorption: Bone resorption normally increases after peak bone mass is reached, but age-related bone resorption may be greater than normal for a variety of reasons. One possible reason is calcium or vitamin D deficiency, which causes the parathyroid gland to release PTH, the hormone that promotes resorption by osteoclasts.
- There is the inadequate formation of new bone by osteoblasts during remodeling: Lack of estrogen may decrease the normal deposition of new bone. Inadequate levels of calcium and vitamin D also lead to the impaired bone formation by osteoblasts.
An imbalance between bone building and bone destruction leading to bone loss may also occur as a side effect of other disorders. For example, people with alcoholism, anorexia nervosa, or hyperthyroidism have an increased rate of bone loss. Some medications — including anti-seizure medications, chemotherapy drugs, steroid medications, and some antidepressants — also increase the rate of bone loss.
Osteoporotic Fractures
Fractures are the most dangerous aspect of osteoporosis, and osteoporosis is responsible for millions of fractures annually. Debilitating pain among the elderly is often caused by fractures from osteoporosis, and it can lead to further disability and early mortality. Fractures of the long bones (such as the femur) can impair mobility and may require surgery. A hip fracture usually requires immediate surgery, as well. The immobility associated with fractures — especially of the hip — increases the risk of deep vein thrombosis, pulmonary embolism, and pneumonia. Osteoporosis is rarely fatal, but these complications of fractures often are. Older people tend to have more falls than younger people, due to such factors as poor eyesight and balance problems, increasing their risk of fractures even more. The likelihood of falls can be reduced by removing obstacles and loose carpets or rugs in the living environment.
Risk Factors for Osteoporosis
There are a number of factors that increase the risk of osteoporosis. Eleven of them are listed below. The first five factors cannot be controlled, but the remaining factors generally can be controlled by changing behaviors.
- older age
- XX chromosome
- European or Asian ancestry
- family history of osteoporosis
- short stature and small bones
- smoking
- alcohol consumption
- lack of exercise
- vitamin D deficiency
- poor nutrition
- consumption of soft drinks
Treatment and Prevention of Osteoporosis
Osteoporosis is often treated with medications that may slow or even reverse bone loss. Medications called bisphosphonates, for example, are commonly prescribed. Bisphosphonates slow down the breakdown of bone, allowing bone rebuilding during remodeling to keep pace. This helps maintain bone density and decreases the risk of fractures. The medications may be more effective in patients who have already broken bones than in those who have not, significantly reducing their risk of another fracture. Generally, patients are not recommended to stay on bisphosphonates for more than three or four years. There is no evidence for continued benefit after this time — in fact, there is a potential for adverse side effects.

Preventing osteoporosis includes eliminating any risk factors that can be controlled through changes of behavior. If you smoke, stop. If you drink, reduce your alcohol consumption — or cut it out altogether. Eat a nutritious diet and make sure you are getting adequate amounts of vitamin D. You should also avoid drinking carbonated beverages.
If you’re a couch potato, get involved in regular exercise. Aerobic, weight-bearing and resistance exercises can all help maintain or increase bone mineral density. Exercise puts stress on bones, which stimulates bone building. Good weight-bearing exercises for bone-building include weight training, dancing, stair climbing, running, and hiking (Figure \(\PageIndex{4}\)). Biking and swimming are less beneficial because they don’t stress the bones. Ideally, you should exercise for at least 30 minutes a day on most days of the week.
Osteoarthritis
Osteoarthritis (OA) is a joint disease that results from the breakdown of joint cartilage and bone. The most common symptoms are joint pain and stiffness. Other symptoms may include joint swelling and decreased range of motion. Initially, symptoms may occur only after exercise or prolonged activity, but over time, they may become constant, negatively affecting work and normal daily activities. As shown in Figure \(\PageIndex{5}\), the most commonly involved joints are those near the ends of the fingers, at the bases of the thumbs, and in the neck, lower back, hips, and knees. Often, joints on one side of the body are affected more than those on the other side.
What Causes Osteoarthritis?
OA is thought to be caused by mechanical stress on the joints with insufficient self-repair of cartilage. The stress may be exacerbated by low-grade inflammation of the joints, as cells lining the joint attempt to remove breakdown products from cartilage in the synovial space. OA develops over decades as stress and inflammation cause an increasing loss of articular cartilage. Eventually, bones may have no cartilage to separate them, so bones rub against one another at joints. This damages the articular surfaces of the bones and contributes to the pain and other symptoms of OA. Because of the pain, movement may be curtailed, leading to loss of muscle, as well.
Diagnosing Osteoarthritis
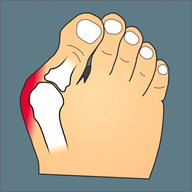
Diagnosis of OA is typically made on the basis of signs and symptoms. Signs include joint deformities, such as bony nodules on the finger joints or bunions on the feet (Figure \(\PageIndex{6}\)). Symptoms include joint pain and stiffness. The pain is usually described as a sharp ache or burning sensation, which may be in the muscles and tendons around the affected joints, as well as in the joints themselves. The pain is usually made worse by prolonged activity, and it typically improves with rest. Stiffness is most common when first arising in the morning, and it usually improves quickly as daily activities are undertaken.
X-rays or other tests are sometimes used to either support the diagnosis of OA or to rule out other disorders. Blood tests might be done, for example, to look for factors that indicate rheumatoid arthritis (RA), an autoimmune disease in which the immune system attacks the body’s joints. If these factors are not present in the blood, then RA is unlikely, and a diagnosis of OA is more likely to be correct.
Risk Factors for Osteoarthritis
Age is the chief risk factor for osteoarthritis. By age 65, as many as 80 percent of all people have evidence of osteoarthritis. However, people are more likely to develop OA — especially at younger ages — if they have had a joint injury. A high school football player might have a bad knee injury that damages the joint, leading to OA in the knee by the time he is in his thirties. If people have joints that are misaligned due to congenital malformations or disease, they are also more likely to develop OA. Excess body weight is another factor that increases the risk of OA, because of the added stress it places on weight-bearing joints.
Researchers have found that people with a family history of OA have a heightened risk of developing the disorder, which suggests that genetic factors are also involved in OA. It is likely that many different genes are needed for normal cartilage and cartilage repair. If such genes are defective and cartilage is abnormal or not normally repaired, OA is more likely to result.
Treatment and Prevention of Osteoarthritis
OA cannot be cured, but the symptoms — especially the pain — can often be treated successfully to maintain a good quality of life for people with OA. Treatments include exercise, efforts to decrease stress on joints, pain medications, and surgery.
Destressing Joints
Efforts to decrease stress on joints include resting and using mobility devices such as canes, which reduce the weight placed on weight-bearing joints and also improve stability. In people who are overweight, losing weight may also reduce joint stress.
Exercise
Exercise helps maintain joint mobility and also increases muscle strength. Stronger muscles may help keep the bones in joints correctly aligned, and this can reduce joint stress. Good exercises for OA include swimming, water aerobics (see Figure \(\PageIndex{7}\)), and biking. These activities are recommended for OA because they put relatively little stress on the joints.

Pain Medications
The first type of pain medication likely to be prescribed for OA is acetaminophen (e.g., Tylenol). When taken as prescribed, it has a relatively low risk of serious side effects. If this medication is inadequate to relieve the pain, non-steroidal anti-inflammatory drugs (NSAIDs, such as ibuprofen) may be prescribed. NSAIDs, however, are more likely to cause serious side effects, such as gastrointestinal bleeding, elevated blood pressure, and increased risk of stroke. Opioids usually are reserved for patients who have suffered serious side effects or for whom other medications have failed to relieve pain. Due to the risk of addiction, the short-term use of opioids is generally recommended.
Surgery
Joint replacement surgery is the most common treatment for serious OA in the knee or hip. In fact, knee and hip replacement surgeries are among the most common of all surgeries. Although they require a long period of healing and physical rehabilitation, the results are usually worth it. The replacement “parts” are usually pain-free and fully functional for at least a couple of decades. Quality, durability, and customization of artificial joints are constantly improving.
About one out of every two Americans will develop osteoarthritis in his or her lifetime. The more you know about this disease, the more you can do to avoid it or slow its progression. That means knowing the facts, rather than believing the myths about osteoarthritis.
Myth: Cracking my knuckles will cause osteoarthritis.
Reality: Cracking your knuckles may lead to inflammation of your tendons, but it will not cause osteoarthritis.
Myth: My diet has no effect on my joints.
Reality: What and how much you eat does affect your body weight, and every pound you gain translates into an additional four pounds (or more!) of stress on your knees. Being overweight, therefore, increases the chances of developing osteoarthritis — and also the rate at which it progresses.
Myth: Exercise causes osteoarthritis or makes it worse, so I should avoid it.
Reality: This is one of the biggest myths about osteoarthritis. Low-impact exercise can actually lessen the pain and improve other symptoms of osteoarthritis. If you don’t have osteoarthritis, exercise can reduce your risk of developing it. Low-impact exercise helps keep the muscles around joints strong and flexible, so they can help stabilize and protect the joints.
Myth: If my mom or dad has osteoarthritis, I will also develop it.
Reality: It is true that you are more likely to develop osteoarthritis if a parent has it, but it isn’t a sure thing. There are several things you can do to decrease your risk, such as getting regular exercise and maintaining a healthy weight.
Myth: Bad weather causes osteoarthritis.
Reality: Weather conditions do not cause osteoarthritis, although, in some people who already have osteoarthritis, bad weather seems to make the symptoms worse. It is primarily low barometric pressure that increases osteoarthritis pain, probably because it leads to greater pressure inside the joints relative to the outside air pressure. Some people think their osteoarthritis pain is worse in cold weather, but systematic studies have not found convincing evidence for this.
Myth: Joint pain is unavoidable as you get older, so there is no need to see a doctor for it.
Reality: Many people with osteoarthritis think there is nothing that can be done for the pain of osteoarthritis, or that surgery is the only treatment option. In reality, osteoarthritis symptoms often can be improved with a combination of exercise, weight loss, pain management techniques, and pain medications. If osteoarthritis pain interferes with daily life and lasts more than a few days, you should see your doctor.
Myth: Osteoarthritis is inevitable in seniors.
Reality: Although many people over 65 develop osteoarthritis, there are many people who never develop it, no matter how old they live to be. You can reduce your risk of developing osteoarthritis in later life by protecting your joints throughout life.
Review
- Name the two most common disorders of the skeletal system.
- What is osteoporosis? What causes it?
- How is osteoporosis diagnosed?
- Why is osteoporosis dangerous?
- Identify risk factors for osteoporosis.
- How is osteoporosis treated? What can be done to prevent it?
- What is OA? What are its chief symptoms?
- What causes OA?
- Describe how OA is diagnosed.
- Identify risk factors for OA.
- How is OA treated?
- Why is it important to build sufficient bone mass in your young adult years?
- Explain the difference in the cause of rheumatoid arthritis and osteoarthritis.
- True or False: Osteoarthritis is caused by physical activity, so people who are equally active are equally susceptible to it.
- True or False: Estrogen generally promotes the production of new bone.
Explore More
Osteoarthritis grinds down millions of joints. Many people find relief from hip or knee pain and disability by having one or more joints replaced with artificial joints made of metal and plastic. In the U.S. alone, more than a million knee and hip joint replacements are performed each year. However, the best remedy for worn out, painful joints is replacement with real biological tissue from a tissue donor rather than replacement with artificial joints. Unfortunately, using human donor tissues to repair joints is very costly. There is also a severe shortage of donor tissues. Orthopedic surgeon and researcher Kevin Stone is developing a treatment that could avoid these drawbacks of human tissue transplants by using specially developed animal tissues. Watch his TED talk to learn more:
Check out this video to learn about Primordial Dwarfism here:
Attributions
- Osteoporosis by Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. licensed CC BY 3.0 via Wikimedia Commons
- Osteoporosis of spine by OpenStax College, CC BY 3.0 via Wikimedia Commons
- Age and bone mass by OpenStax College, CC BY 3.0 via Wikimedia Commons
- Hikers enjoying a wild trail by Hillebrand Steve, U.S. Fish and Wildlife Service, public domain via Wikimedia Commons
- Areas affected by osteoarthritis by US Federal Government, public domain via Wikimedia Commons
- Hallux valgus by Malmstajn, CC BY 3.0 via Wikimedia Commons
- Water aerobics by Tim Ross, public domain via Wikimedia Commons
- Text adapted from Human Biology by CK-12 licensed CC BY-NC 3.0