
4.5: Obesity
- Page ID
- 16736

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Everybody needs food energy just to stay alive, but too much energy consumption, coupled with too little energy use, is too much of a good thing. People who consistently consume more food energy than they use may become obese like the woman pictured here.

What Is Obesity?
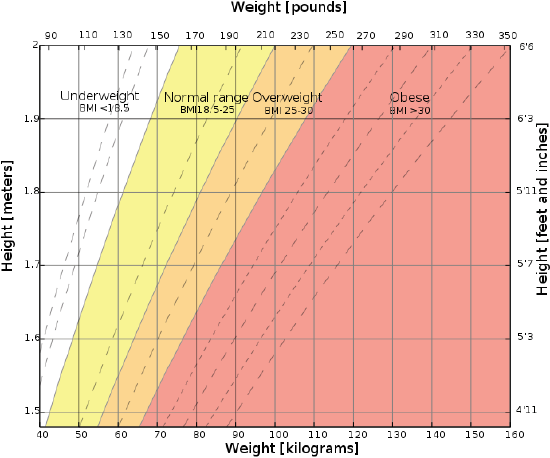
Obesity is a disease in which excess body fat has accumulated to the extent that it is likely to have negative effects on health. Obesity is commonly diagnosed on the basis of the body mass index (BMI). BMI is an estimate of body fatness based on a person’s weight relative to their height. BMI is calculated by dividing a person’s weight (in kilograms) by the square of the person’s height (in meters). The graph below shows how BMI is used to categorize obesity and other body mass classes for adults. A BMI value of 18.5 to 25 kg/m2 is considered normal. A BMI below 18.5 kg/m2 is considered underweight. A BMI between 25 and 30 kg/m2 places a person in the overweight range. A BMI greater than 30 kg/m2 classifies a person as obese.
Obesity in children and adolescents is generally defined not simply by BMI but by comparison of BMI with reference values. Obesity is diagnosed when a child has a BMI that is greater than the 95th percentile of the reference values for children of the same age. This means that the child’s BMI is higher than that of 95 percent of same-aged children in the reference sample. The reference values are based on large samples of children from the mid-to-late 20th century, before the recent rise in childhood obesity.
Categories of Obesity
The medical profession breaks down obesity into additional categories, although the exact delineation of the categories is not universally agreed upon. Commonly accepted categories include:
- severe obesity, which is diagnosed when a person has a BMI ≥ 35 kg/m2.
- morbid obesity, which is diagnosed when a person has a BMI ≥ 35 kg/m2 and obesity-related health problems, or when a person has a BMI ≥ 40 kg/m2 but < 45 kg/m2.
- super obesity, which is diagnosed when a person has a BMI ≥ 45 kg/m2
Fat Distribution in Obesity
Obesity can also be categorized in terms of fat distribution, as measured by waist-to-hip ratio (waist circumference divided by hip circumference). A waist-to-hip ratio greater than 0.85 for women or 0.90 for men is diagnostic of central obesity, in which most of the excess fat is stored in the abdomen. This type of fat distribution gives a person an apple shape, like the man pictured above. People with central obesity are at greater risk of the adverse health consequences of obesity than people who store most of their excess fat around the hips (giving them a pear shape). Because it accounts for the elevated risks associated with central obesity, waist-to-hip ratio is a better predictor than BMI of mortality in older obese patients
Causes of Obesity
Like many other diseases, most cases of obesity are the result of an interplay between genetic and environmental factors. Obesity is most commonly caused by a combination of excessive food intake, inadequate physical activity, and genetic susceptibility.
Genetic Influences on Obesity
Various genes that control appetite and metabolism predispose people to develop obesity when sufficient food energy is present. It is likely that dozens of such genes exist. Family studies reveal the strength of the genetic influence on obesity. When both parents are obese, 80 percent of their offspring will also be obese. For comparison, when both parents are of normal weight, less than 10 percent of their offspring will be obese.
Diet and Obesity
From 1971 to 2000 in the United States, the average amount of food consumed by women actually increased by 335 Calories per day, and by men by 168 Calories per day. During the same period, the rate of obesity in U.S. adults increased from about 15 to 31 percent. Most of the extra food energy came from an increase in carbohydrate consumption. Primary sources of these extra carbohydrates were sugar-sweetened beverages, like those pictured below. Sugary beverages include not only soft drinks but also fruit drinks, sweetened iced tea and coffee, and energy and vitamin water drinks. Such drinks now account for almost 25 percent of daily food energy in young adults in the United States. This is an alarming statistic, given that these drinks provide no other nutrients except energy.
Activity Levels and Obesity
A sedentary lifestyle plays a significant role in obesity. Worldwide, there has been a large shift toward less physically demanding work. There has also been an increased reliance on cars and labor-saving devices at home. Currently, an estimated 30 percent of the world’s population gets insufficient exercise.
Other Causes of Obesity
A minority of cases of obesity are caused by certain medications or by other diseases. Medications that may increase the risk of obesity include antidepressant and antipsychotic drugs, steroids such as prednisone, and some forms of hormonal contraception, among others. Diseases that increase the risk of obesity include hypothyroidism, Cushing’s disease, binge eating disorder, and Prader-Willi syndrome.
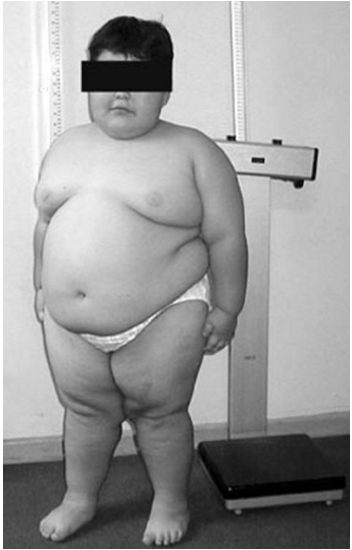
Consider Prader-Willi syndrome as an example. A young child with this syndrome is shown in Figure \(\PageIndex{3}\). The syndrome occurs due to the loss of function of specific genes on chromosome 15. Symptoms of the syndrome include constant hunger, which typically leads to severe obesity in childhood. Prader-Willi syndrome is caused by genetic defects but it is not generally inherited. Instead, the genetic changes happen during the formation of the egg or sperm or during embryonic development.
Pathophysiology of Obesity
A recently proposed physiological mechanism for the development of obesity is leptin resistance. Leptin is called the satiety hormone. It is secreted by fat cells and helps to regulate appetite based on the body’s fat reserves. When fat reserves are high, more leptin is secreted and appetite is inhibited, so you eat less. The opposite occurs when fat reserves are low. In obesity, decreased sensitivity to leptin occurs, resulting in an inability to detect satiety despite high-fat reserves. As a consequence, people with leptin resistance never feel satiated and are likely to overeat and gain more weight.
Health Consequences of Obesity
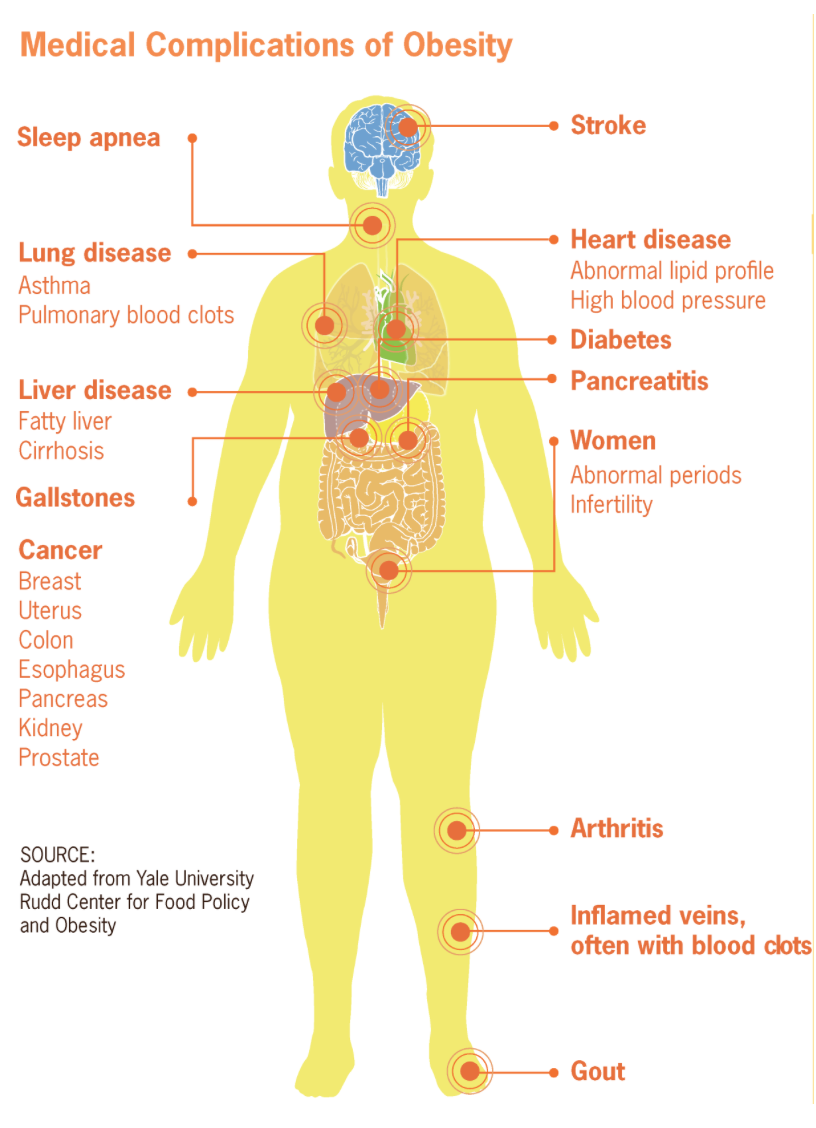
As shown in Figure \(\PageIndex{4}\), obesity increases the risk of many health problems and diseases, including:
- sleep apnea
- lung disease, asthma, pulmonary blood clots
- liver disease, fatty liver, cirrhosis
- gallstones
- cancer of breast, uterus, colon, esophagus, pancreas, kidney, prostate
- stroke
- heart disease, abnormal lipid profile, high blood pressure
- diabetes
- pancreatitis
- abnormal periods and infertility
- arthritis
- inflamed veins often with blood clots
- gout
The health consequences of obesity are mainly due to the effects of either increased fat mass or increased numbers of fat cells. Extra weight from excess body fat places a lot of stress on the body and its organ systems, causing diseases such as osteoarthritis and obstructive sleep apnea. An increased number of fat cells increases inflammation and the risk of blood clots. It also changes the body’s metabolism, altering the body’s response to insulin and potentially leading to insulin resistance and type 2 diabetes. This explains why the link between obesity and type 2 diabetes is so strong. Obesity is thought to be the root cause of 64 percent of cases of type 2 diabetes in men and 77 percent of cases in women.
Not surprisingly, obesity has been found to reduce life expectancy. On average, obesity reduces life expectancy by six or seven years. Super obesity reduces life expectancy by as much as ten years.
Treating and Preventing Obesity
Most cases of obesity are treatable or preventable through changes in diet and physical activity that restore energy balance to the body. In fact, obesity is one of the leading preventable causes of disease and death worldwide. The amount of energy provided by the diet can be reduced by decreasing consumption of energy-dense (high-Calorie) foods, such as foods high in fat and sugar, and increasing consumption of high-fiber foods. The fiber in the diet cannot be digested, so it adds bulk and a feeling of fullness without adding Calories. All types of low-carbohydrate and low-fat diets appear equally beneficial in reducing obesity and its health risks. In some cases, medications may be prescribed to help control obesity by reducing appetite or fat absorption.
Bariatric Surgery
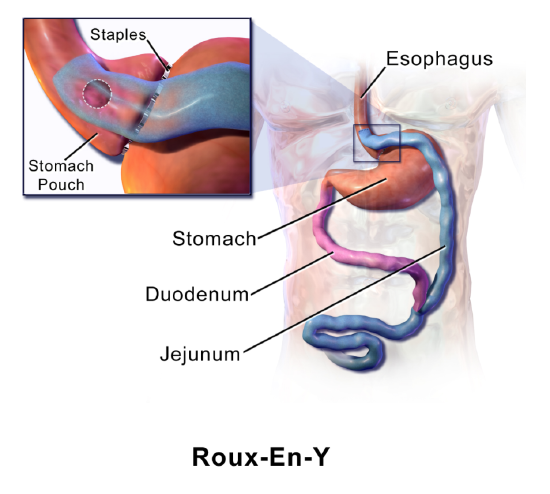
If changes in diet and exercise and even medications are not effective, bariatric surgery may be recommended as a treatment for obesity. Bariatric surgery is the single most effective medical treatment for obesity. There are several different types of bariatric surgery, one of which is illustrated in figure \(\PageIndex{5}\). In this particular type of surgery, the size of the stomach is greatly reduced so less food can be eaten at a time. The length of the small intestine is also reduced so fewer nutrients can be absorbed from food.
Public Health Approaches
Public health approaches to the problem of obesity include efforts to understand and correct the environmental factors responsible for increasing obesity rates. The goals are to reduce food energy consumption and promote energy expenditure in physical activity. Efforts to reduce energy consumption include promoting healthy meals and limiting access to sugary beverages and junk foods in schools. Efforts to promote physical activity include increasing access to parks and developing pedestrian routes in urban environments.
Review
- Define obesity.
- How is obesity generally diagnosed in adults? In children?
- Compare and contrast severe obesity, morbid obesity, and super obesity.
- What is central obesity? What is its relationship to the adverse health consequences of obesity?
- Give examples of medications and disorders that may cause obesity.
- Discuss factors that cause most cases of obesity.
- What is leptin resistance, and what is its connection with obesity?
- Identify some of the health consequences of obesity.
- Describe types of treatments available for obesity.
- Describe public health approaches to treating and preventing obesity.
- Which is likely to be worse for a person’s health — having their hip circumference be larger than their waist circumference, or vice versa? Explain your answer.
- What factors is BMI based on?
- Why is the recent increase in childhood obesity a public health concern?
Explore More
Watch this video to learn which is better for losing weight, diet or exercise:
Check out this video to learn about body mass index (BMI) and why it might not be the best measurement for obesity:
Attributions
- Obesidad en Mexico by Mallinaltzin, CC BY 3.0 via Wikimedia Commons
- Body mass index chart by InvictaHOG, public domain via Wikimedia Commons
- PWS8 by Fanny Cortés M1, M. Angélica Alliende R1,a, Andrés Barrios R1,2, Bianca Curotto L1,b, Lorena Santa María V1,c, Ximena Barraza O3, Ledia Troncoso A2, Cecilia Mellado S4,6, Rosa Pardo V, CC BY 4.0 via Wikimedia Commons
- Medical complications of obesity by CDC, public domain via Wikimedia Commons
- Roux-En-Y by Blausen.com staff (2014). "Medical gallery of Blausen Medical 2014". WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. licensed CC BY 3.0 via Wikimedia Commons
- Text adapted from Human Biology by CK-12 licensed CC BY-NC 3.0