
15.1.1.4: Mycobacterium tuberculosis
- Page ID
- 42654
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)

Organism
- Mycobacterium tuberculosis is a large Gram-positive, acid fast bacillus. It does not form endospores. (Figure \(\PageIndex{2}\))
- The cultured bacilli often form “cords” which are bundles of streptobacilli
- Typically considered a strict aerobe
- Grows very slowly
- Sometimes called the “tubercle bacillus”

Habitat
- The natural reservoir of M. tuberculosis is infected individuals
- Because of the waxy layer of its acid fast cell wall, M. tuberculosis can remain in the environment for months after being released by an infected individual in respiratory droplets
- Its waxy cell wall also makes it more difficult to kill with disinfectants than other non-sporeforming Gram-positives
Source
- Inhaled or otherwise enters the respiratory tract
Epidemiology
- Almost a quarter of the world’s population is infected with M. tuberculosis, although it is asymptomatic in most cases
- Spreads easily among people living in close quarters
- People with other diseases, poor nutrition, or weak immune systems are most at risk for severe disease and death
Clinical Disease
- M. tuberculosis causes tuberculosis or TB (sometimes referred to as “consumption” historically)
- Begins as a respiratory infection, but can spread to any part of the body, including the liver, bones, and brain
- Tuberculosis occurs in stages (Figure \(\PageIndex{3}\))
- Primary tuberculosis
- The bacterium is inhaled and engulfed by macrophages in the lung
- The macrophages are unable to destroy the M. tuberculosis due to its waxy cell wall
- The M. tuberculosis grows within the macrophages in the lung. Some of the macrophages lyse and release the bacteria which are also engulfed by macrophages
- B- and T-cells are recruited to the site of infection but cannot destroy the M. tuberculosis cells
- The area is walled off by the immune system in a fibrin-containing structure to contain the infection. In general, these structures are called “granulomas”, but in this specific case they are called “tubercles” (thus “tuberclosis”).
- The center of the tubercles form what is referred to as “caseous necrosis” (“caseous” means “cheesy”) which consists of the M. tuberculosis, dead tissue, and immune cells.
- Most M. tuberculosis infections are halted by the formation of tubercles and the person remains asymptomatic
- Secondary or reactivated tuberculosis
- If the infected person has a weakened immune system, malnutrition or other disease, the tubercles can rupture and release the M. tuberculosis which had been contained
- Anywhere the released bacteria land in the body, new tubercles are formed. Although this is primarily in the lungs, tubercles can form anywhere in the body.
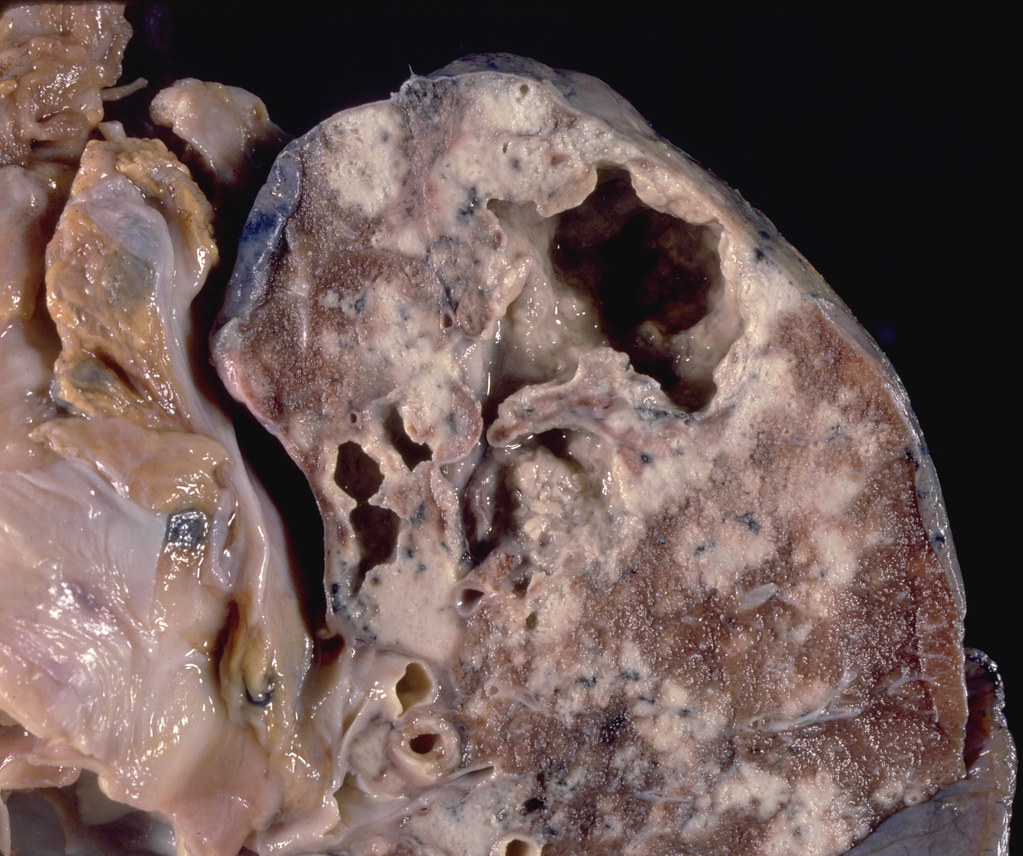
- The tubercles and their rupture cause tissue damage and subsequently reduced lung function (and/or function of other organs/tissues containing tubercles) (Figure \(\PageIndex{4}\))
- Symptoms of active TB include:
- Coughing that lasts three or more weeks
- Coughing up blood
- Chest pain, or pain with breathing or coughing
- Unintentional weight loss
- Fatigue
- Fever
- Night sweats
- Chills
- Loss of appetite

- Antibiotics used to treat TB are usually isoniazid (INH), rifampin (RIF), and pyrazinamide (PZA) and ethambutol (EMB) or streptomycin (SM). These are used in combination to prevent development of antibiotic resistance, which is of particular concern in M. tuberculosis.
- It can be difficult to keep patients compliant with treatment.
- Because of the slow growth of M. tuberculosis the treatment course is very long (6-9 months)
- The side effects of these antibiotics can be unpleasant
- Patients are often asymptomatic when they begin treatment
- Public health officials sometimes use directly observed therapy (DOT) to ensure compliance
- Many strains of M. tuberculosis are now resistant to multiple drugs (MDR-TB). Some are resistant to most of the first- and second-line antibiotics (XDR-TB)
- There is a vaccine available (the BCG vaccine), but it is not particularly effective and is not used in the United States
Primary Virulence Factors
- Mycobacterium tuberculosis does not produce any toxins or exoenzymes which damage tissue
- The protective waxes in the cell wall which prevent destruction by the immune system are the primary virulence factor of M. tuberculosis
- The damage caused in the course of tuberculosis is a result of the immune response to M. tuberculosis
Additional Information: