
5.10: Infertility
- Page ID
- 187722

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)This family portrait in Figure \(\PageIndex{1}\) shows that human societies value having children. Indeed, for most people, parenthood is an important life goal. Unfortunately, some people are unable to achieve that goal because of infertility.

Figure \(\PageIndex{1}\): Family portrait Taylor McKenzie Flickr CC-BY-SA 2.0
What Is Infertility?
Infertility is the inability of a sexually mature adult to reproduce by natural means. For scientific and medical purposes, infertility is generally defined as the failure to achieve a successful pregnancy after at least one year of regular, unprotected sexual intercourse. Infertility may be primary or secondary. Primary infertility applies to cases in which an individual has never achieved a successful pregnancy. Secondary infertility applies to cases in which an individual has had at least one successful pregnancy, but fails to achieve another after trying for at least a year. Infertility is a common problem. About ten percent (6.1 million) of U.S. women aged 15 to 44 have difficulty getting or staying pregnant.
Causes of Infertility
Pregnancy is the result of a multi-step process. For a normal pregnancy to occur, an egg must be released from one of the ovaries, travel through a Fallopian tube, be fertilized by a sperm as it passes through the tube, and then implant in the uterus. If there is a problem with any of these steps, infertility can result.
Causes of Male Infertility
Male infertility occurs when there are no or too few sperm, or when the sperm are not healthy and motile and cannot travel through the female reproductive tract to fertilize an egg. A common cause of inadequate numbers or motility of sperm is varicocele, which is an enlargement of blood vessels in the scrotum. This may raise the temperature of the testes and adversely affect sperm production. In other cases, there is no problem with the sperm, but there is a blockage in the male reproductive tract that prevents the sperm from being ejaculated.
Factors that increase a man’s risk of infertility include heavy alcohol use, drug abuse, cigarette smoking, exposure to environmental toxins (such as pesticides or lead), certain medications, serious diseases (such as kidney disease), and radiation or chemotherapy for cancer. Another risk factor is advancing age. Male fertility normally peaks in the mid-twenties and gradually declines after about age 40, although it may never actually drop to zero.
Causes of Female Infertility
Female infertility generally occurs due to one of two problems: failure to produce viable eggs by the ovaries or structural problems in the Fallopian tubes or uterus. The most common cause of female infertility is a problem with ovulation. Without ovulation, there are no eggs to be fertilized. Anovulatory cycles (menstrual cycles in which ovulation does not occur) may be associated with no or irregular menstrual periods, but even regular menstrual periods may be anovulatory for a variety of reasons. The most common cause of anovulatory cycles is polycystic ovary syndrome (PCOS), which causes hormone imbalances that can interfere with normal ovulation. Another relatively common cause of anovulation is primary ovarian insufficiency. In this condition, the ovaries stop functioning normally and producing viable eggs at a relatively early age, generally before age 40.
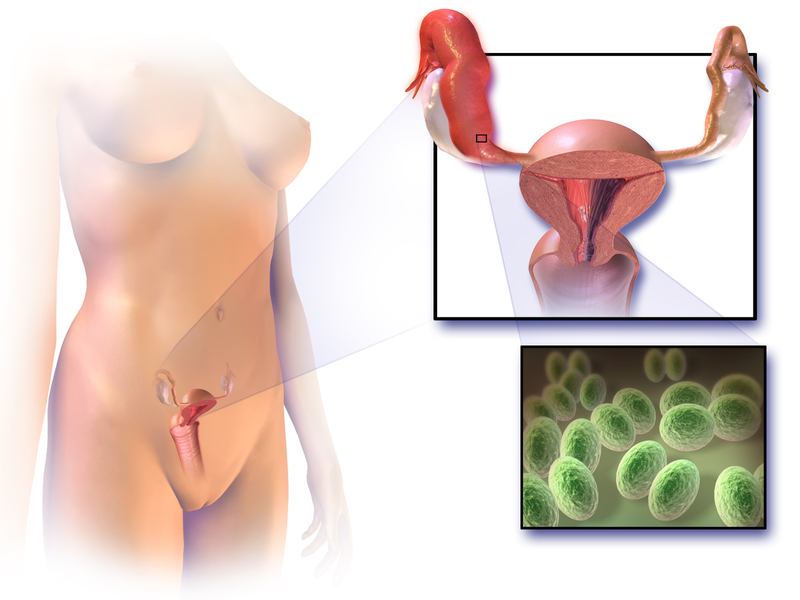
Structural problems with the Fallopian tubes or uterus are less common causes of infertility. The Fallopian tubes may be blocked as a result of endometriosis. Another possible cause is a pelvic inflammatory disease, which occurs when sexually transmitted infections spread to the Fallopian tubes or other female reproductive organs (Figure \(\PageIndex{2}\)). The infection may lead to scarring and blockage of the Fallopian tubes. If an egg is produced and the Fallopian tubes are functioning — and a woman has a condition such as uterine fibroids — implantation in the uterus may not be possible. Uterine fibroids are non-cancerous clumps of tissue and muscle that form on the walls of the uterus.
Factors that increase a woman’s risk of infertility include tobacco smoking, excessive use of alcohol, stress, poor diet, strenuous athletic training, and being overweight or underweight. Advanced age is even more problematic for women than for men. Female fertility normally peaks in the mid-twenties and declines continuously after age 30, until menopause around age 52, after which the ovary no longer releases eggs. About one-third of couples in which the woman is over age 35 have fertility problems. In older women, more cycles are likely to be anovulatory, and the eggs may not be as healthy.
Diagnosing Causes of Infertility
Diagnosing the cause(s) of a couple’s infertility often requires testing both partners for potential problems. The semen is likely to be examined for sperm count, shape, and motility. If problems are found with sperm, further studies are likely to be done, such as medical imaging to look for structural problems with the testes or ducts.
In individuals with ovaries and a uterus, the first step is most often determining whether ovulation is occurring. This can be done at home by carefully monitoring body temperature (which rises slightly around the time of ovulation) or by using a home ovulation test kit, available over the counter at most drugstores. Whether or not ovulation is occurring can also be detected with blood tests or ultrasound imaging of the ovaries. If ovulation is occurring normally, the next step may be an X-ray of the Fallopian tubes and uterus to look for blockages or other structural problems. Another approach to examining the reproductive tract for potential problems is laparoscopy. In this surgical procedure, a tiny camera is inserted into the abdomen through a small incision. This allows the doctor to directly inspect the reproductive organs.
When it comes to making a baby, we know it takes two to tango. So why do the pressures of fertility often fall on only one half of the equation? In this video, data journalist Mona Chalabi examines some of the big misconceptions about fertility, highlights significant blind spots in the data, and explains why we need more research on sperm.
Treating Infertility
Infertility often can be treated successfully. The type of treatment depends on the cause of infertility.
Treating Male Infertility
Medical problems that interfere with sperm production may be treated with medications or other interventions that may lead to the resumption of normal sperm production. For example, if an infection is interfering with sperm production, antibiotics may resolve the problem. If there is a blockage in the ejaculation of sperm, surgery may be able to remove the blockage. Alternatively, the sperm may be removed from his body and then used for the artificial insemination of their partner. In this procedure, the sperm are injected into the uterus.
Treating Female Infertility
It is possible to correct blocked Fallopian tubes or uterine fibroids with surgery. Ovulation problems, on the other hand, are usually treated with hormones that act either on the pituitary gland or on the ovaries. Hormonal treatments that stimulate ovulation often result in more than one egg being released at a time, increasing the chance of conceiving twins, triplets, or higher-order multiple births. Multiple fetuses are at greater risk of being born too early or having health and developmental problems. The mother is also at greater risk of complications arising during pregnancy. Therefore, the possibility of multiple fetuses should be weighed in making a decision about this type of infertility treatment.
Assisted Reproductive Technology
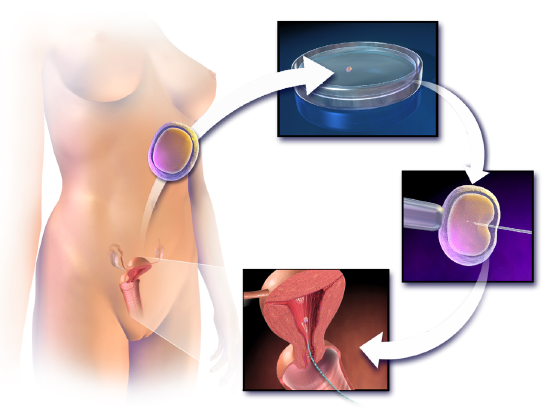
Some cases of infertility are treated with assisted reproductive technology (ART). This is a collection of medical procedures in which eggs and sperm are removed and manipulated to increase the chances of fertilization. The eggs and sperm may be injected into one of the Fallopian tubes for fertilization to take place in vivo (in the body). More commonly, however, the eggs and sperm are mixed together outside the body so fertilization takes place in vitro (in a test tube or dish in a lab). The latter approach is illustrated in Figure \(\PageIndex{3}\). With in vitro fertilization, the fertilized eggs may be allowed to develop into embryos before being placed in the woman’s uterus.
ART has about a 40 percent chance of leading to a live birth in women under the age of 35, but only about a 20 percent chance of success after the age of 35. Some studies have found a higher-than-average risk of birth defects in children produced by ART procedures, but this may be due to the generally higher ages of the parents, not the technologies used. Same-sex couples take advantage of the ART process to expand their family.
Infertility affects 1 in 8 couples worldwide. But in the last 40 years, more than 5 million babies have been born using in vitro fertilization (IVF). How does it work? Nassim Assefi and Brian A. Levine detail the science behind making a baby in a lab.
Other Approaches
Other approaches for certain causes of infertility and same-sex couples include the use of a surrogate mother, a gestational carrier, or sperm donation.
- A surrogate mother is a woman who agrees to become pregnant using the man’s sperm and her own egg. The child, who will be the biological offspring of the surrogate and the male partner, is given up at birth for adoption by the couple. Surrogacy might be selected by women with no eggs or eggs that are unhealthy. A woman who carries a mutant gene for a serious genetic disorder might choose this option to ensure that the defective gene is not passed on to her offspring.
- A gestational carrier is a woman who agrees to receive a transplanted embryo from a couple and carry it to term. The child, who will be the couple's biological offspring, is given to the parents at birth. A gestational carrier might be used by women who have normal ovulation but no uterus, or who cannot safely carry a fetus to term because of a serious health problem (such as kidney disease or cancer). This method is commonly used by gay men couples.
- Sperm donation is the use of sperm from a fertile man (generally through artificial insemination) for cases in which the male partner in a couple is infertile, or in which a woman seeks to become pregnant without a male partner. A lesbian couple may use donated sperm to enable one of them to become pregnant and have a child. Sperm can be obtained from a sperm bank, which buys and stores sperm for artificial insemination, or a male friend or another individual may donate sperm to a specific woman.
More than 14 million people in the United States have polycystic ovary syndrome (PCOS), an endocrine disorder with a genetic basis that is the most common cause of infertility. Most patients with PCOS have many small cysts on their ovaries. The cysts are not usually harmful, but they lead to hormone imbalances, such as higher-than-normal levels of testosterone in affected individuals. The hormonal imbalances are the primary cause of infertility associated with PCOS. The disorder also increases the risk of a whole slew of other serious health problems, including endometrial cancer, heart disease, high blood pressure, type 2 diabetes, asthma, obesity, depression, and anxiety.
Despite the prevalence of PCOS and its serious potential effects, until recently, its cause was poorly understood. There were also no effective early diagnostic or treatment strategies for it. All that appears to be changing now. A review of the research literature on PCOS published in 2016 provides new insights into its causes, diagnosis, and treatment.
Among the research cited in the review is promising new work on nonhuman animal models, including monkeys and mice. One line of research suggests that PCOS may be programmed into a fetus during the second trimester of pregnancy. Another line of research indicates that hair taken from an infant can be analyzed for early risk factors for PCOS, even though PCOS symptoms do not show up until puberty. In addition, the research is helping scientists identify a constellation of genes that are suspected to play a role in PCOS.
The new research on PCOS is important for those who suffer from the disorder and its consequences, including infertility and life-threatening chronic conditions (such as heart disease and diabetes). The hope is that such research will lead to new ways of diagnosing PCOS at an early age, when medical interventions and lifestyle choices may be used to head off the more serious complications. It is likely that the research will also eventually lead to new and more effective treatment options for the millions of people who battle PCOS